Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


The Covid-19 pandemic has had a devastating impact on UK cancer services with huge numbers of delayed treatments due to the pressure on the NHS. Many patients, particularly older people, were also reluctant to seek medical care during the past 18 months, which has in-turn affected cancer stage diagnoses and survival rates.
The Covid-19 pandemic has had a devastating impact on UK cancer services with huge numbers of delayed treatments due to the pressure on the NHS. Many patients, particularly older people, were also reluctant to seek medical care during the past 18 months, which has in-turn affected cancer stage diagnoses and survival rates.
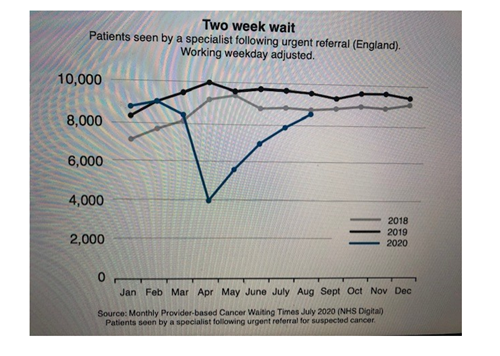
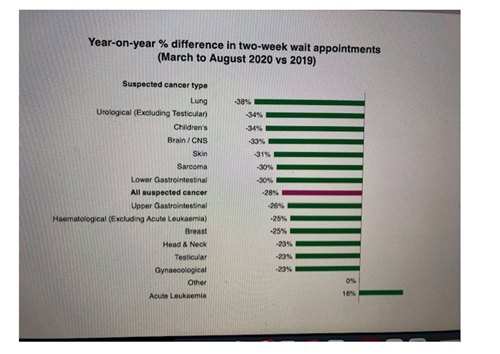
During the pandemic, the numbers of urgent referrals made from primary care significantly reduced, as well as non-urgent referrals from other services, such as respiratory medicine and out-patient clinics.
Population screening was paused and a lot of older people who were eligible for screening were shielding or too afraid to visit their GP or a hospital in case they caught Covid.
This combination of factors means that many patients are missing a primary diagnosis. In fact, there were approximately 50,000 less primary diagnoses of cancer in 2020 compared to 2019. Sadly, this is not because less people are developing cancer, but instead means there are 50,000 ‘missing’ patients who are awaiting a diagnosis.
There have also been significant delays for patients receiving their first treatment, with increasing numbers of people waiting for more than 62 and 104 days. Patients have also had to wait longer for follow-up treatments such as surgery, chemotherapy and radiotherapy. In fact, in May 2020, chemotherapy appointments were only at 70% of normal levels.
Social distancing laws also meant that many cancer patients had to attend investigations or treatment on their own or attend virtual appointments. However, this posed challenges for older patients who are less likely to have access to the technology required and more likely to have visual impairment or auditory issues.
These issues have affected a large proportion of cancer patients. According to the latest figures:
Clearing this backlog of cancer patients awaiting diagnosis and treatment will require time and extra resources. According to the latest estimates, if all services work at pre-pandemic levels plus 10%, it would take 20 months to clear the backlog of patients who missed out on a primary diagnosis. If this number increases to 20%, it would take 11 months.
To clear the backlog of those awaiting treatment, it would take services 17 months if services worked at pre-pandemic levels plus 10%, or 12 months at plus 20%.
Aerosol generating procedures for diagnosis, such as bronchoscopy, were particularly badly affected due to the high risk of spread of infection from airborne droplets.
Respiratory medicine and intensive care units were also badly hit due to the overwhelming number of Covid-19 cases. A lack of beds in intensive care meant that many patients who needed larger cancer surgeries were unable to have procedures performed.
There was also less specialist cancer care available due to the redeployment of oncology staff onto general medical wards.
People with dementia were affected both mentally and physically during the Covid-19 pandemic. Firstly, since patients with dementia account for 69% of care home residents, many suffered long bouts of isolation when visitors were not permitted, impacting on the mental health of the patient as well as their loved ones.
People with dementia are also at an increased risk of their cancer being diagnosed at an unknown stage, which puts these patients at higher risk of negative outcomes. This is because patients with dementia are often not properly investigated; geriatricians and GPs should therefore make sure to undertake comprehensive examinations during medical appointments so cancers are not missed.
Another important thing to consider is whether cancer patients with dementia have the capacity to make decisions about their treatment. After a capacity assessment, the doctor must decide whether the patient is able to give proper, informed consent. If the patient can consent, staff should support and enable their patient. However, if the patient has limited capacity and cannot properly consent, then the main focus should be on supporting and enabling their carer.
Listening to the patient and ensuring good communication is key to improving patient care. One-to-one consultations are valuable and help to achieve the best outcome for the individual.
Language choices are extremely important and should be carefully considered. Ultimately, the patient wants: the truth, equal access to therapy, choice of therapy, multidisciplinary input to support time to decide, and decision-making on clinical grounds, not by age.
Involving the patient in the decision-making process is therefore extremely important. Clinicians must ensure that the patient is adequately informed on their proposed treatment plans and on their own disease status and prognosis.
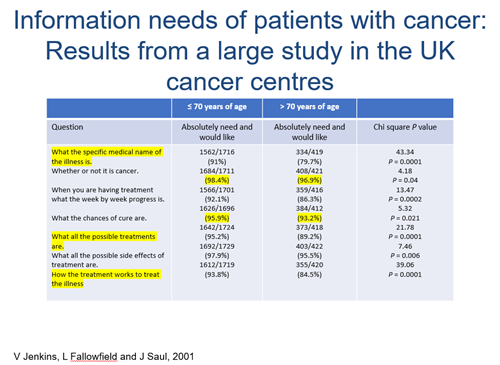
There is a misconception that older patients do not want to know the details of their prognosis, such as whether their cancer is curable. However, a recent information needs study from a UK Cancer Centre found that 96.9% of patients aged 70+ wanted to know whether they had cancer or not, and 93.2% wanted to know what the chances of a cure are.
For those who resist being involved in the decision-making process, a number of simple interventions can help. These include: question prompt sheets, audio-taping of consultations to send to the patient and their family members, and patient decision aids.
GPs and geriatricians should work closely with both the patient and the carer and respect their decisions, such as where the patient wants to spend the rest of their life. When discussing end of life care, geriatricians should always ask and not presume, consider whether the person lives alone, the distance from their family and the social environment.
Doctors must also ensure that the ‘hidden areas’ of getting older and not forgotten. For example: half of people aged 75 and over live alone; one in 10 have less than monthly contact with friends, family and neighbours; and 20% find it difficult to get to their local hospital. Geriatricians should take these factors into account and act accordingly.
They should also consider the position of the carer, including the cost of care, their awareness and knowledge of cancer, whether they have support available and whether there is any unresolved family conflict. Older carers are likely to struggle more completing day-to-day tasks if they are less physically able they should be offered extra support.
Geriatricians and oncologists should also be aware of when to stop therapy or not start therapy, when risk is greater than benefit. Patients should be involved in these conversations with frank and honest discussions about the therapy, as well as the side effects and prognosis.
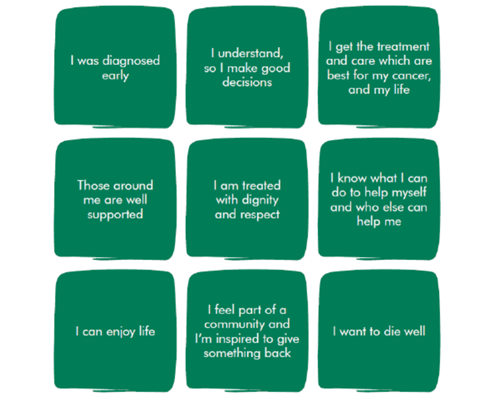
Macmillan highlight nine important areas of focus to ensure the cancer patient has the best possible quality of life. The patient should: be diagnosed early, helped to make informed decisions, receive the best possible treatment and care, have family and friends that are well-supported, treated with dignity and respect, informed about their care and support options, enjoy their life, feel part of the community, and die well.
Ultimately, geriatricians and GPs in cancer care should:
Professor Margot Gosney is an Honorary Consultant in elder care at the Royal Barker NHS Trust and is trained in medical oncology.
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...