Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


The older population is increasing worldwide due to advances in medical technology and new treatment options, which has led to an rise in life expectancy.1 Ageing is associated with decline in physical and cognitive function that results in various health issues such as sarcopenia, falls and frailty.2,3
These health issues limit our ability to be independent in normal activities of daily living and cause decline in our quality of life. For example, approximately one‐third of older adults fall at least once a year4 and a median of 4.1% of falls results in fractures.5
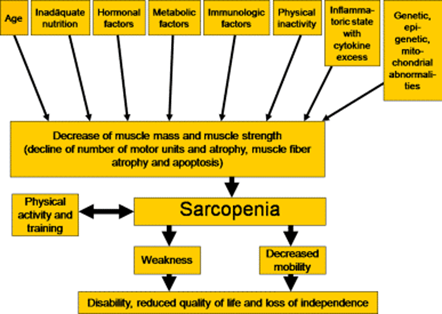
Sarcopenia is defined as “a progressive and generalised skeletal muscle disorder involving the accelerated loss of muscle mass and function that is associated with increased adverse outcomes including falls, fractures, disability, and mortality”.6 There is also a close relationship between sarcopenia, bone loss, or hip fractures called osteo-sarcopenia.7
Sarcopenia is prevalent between 2% and 37% in community‐dwelling older adults, depending on the sarcopenia definition applied8 and associated with decreased mobility, impaired standing balance, functional decline, hospitalisation, and mortality.9
There is age-associated decline in the skeletal muscle mass and strength which starts from approximately the fifth decade of life.10 There is decrease in the muscle mass at a rate of 1 to 2% every year after the age of 50.11 The decline is more rapid afterwards in the sixth and seventh decade of life. These morphological changes are reflected in muscle function.
Muscle strength decreases approximately 20–40% in individuals around age 70 compared to young adults of age 20. The loss of muscle strength even increases to 50% in individuals in their nineties.12
From a histological standpoint, the skeletal muscle consists of type I and type II fibers. Type II fast fibers possess a higher glycolytic potential, lower oxidative capacity, and faster response, whereas type I slow fibers are known as fatigue-resistant due to their characteristics such as greater density and content of mitochondria, capillaries, and myoglobin. There is predominant atrophy of type II fibers in sarcopenia along with smaller and fewer mitochondria.13
The pathological process is multifactorial, and the following changes contribute to development of sarcopenia in old age.
There is increased production of cytokines that have catabolic effects such as IL1, IL6 and TNF alpha14 and the concentration of anabolic cytokines such as IGF-1 is reduced.15
There is a reduction in the level of anabolic hormones such as testosterone, growth hormone, and DHEA and an increase in the level of catabolic hormones e.g. glucocorticoids, myostatin (“myokine” or a hormone-like protein [cytokine] released from muscle, that can act in an autocrine or paracrine fashion).
There is a role of nutritional deficiency and physical inactivity in the development of sarcopenia. Vitamin D deficiency is also widely prevalent in the older population group especially in long-term care institutions such as nursing and residential home facilities.
Vitamin D deficiency is associated with sarcopenia, muscle weakness and reduced physical performance.16 There is emerging evidence that suggests dietary protein supplementation above the recommended dietary amount may be an intervention target to prevent and/or mitigate sarcopenia along with resistance exercise therapy.
Two categories of sarcopenia ‒ primary and secondary ‒ have been recognised in the literature.17
Sarcopenia is either age-related, or primary, when no other specific cause is evident.
It is secondary when causal factors other than ageing are evident. Factors possibly contributing to secondary sarcopenia include physical inactivity owing to limited mobility, disease-related bedrest, or a sedentary lifestyle; poor nutrition owing to undernutrition, inadequate intake of energy or proteins, limited ability to eat, malabsorption or anorexia; and a systemic disease, such as an inflammatory condition (e.g. osteoarthritis, organ failure) or a neurological disorder.
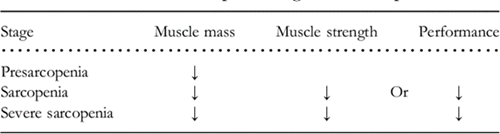
There are two subcategories of sarcopenia:
The European Working Group on Sarcopenia identifies three stages of sarcopenia:
Screening for sarcopenia
Sarcopenia can be identified early through use of fast-screening tools such as the SARC-F questionnaire. This is the easiest available measure for screening in the clinic and requires no special equipment. It has been recommended for screening for sarcopenia by the European Working Group on Sarcopenia in Older People.
SARC‐F includes five components: strength, assistance walking, rise from a chair, climb stairs, and falls. SARC‐F items were selected to reflect health status changes associated with the consequences of sarcopenia.18
Scores range from 0-10, with 0-2 for each component.7 Participants with total score higher than 4 are classified as having sarcopenia. Details of SARC-F are shown below.
Strength
How much difficulty do you have in lifting and carrying 10 pounds?
Assistance in walking
How much difficulty do you have in walking across a room?
Rise from a chair
How much difficulty do you have in transferring from a chair or bed?
Climb stairs
How much difficulty do you have in climbing a flight of 10 stairs?
Falls
How many times have you fallen in the past 1 year?
A score equal to or greater than 4 is predictive of sarcopenia and poor outcomes.
Diagnosis of sarcopenia is based on documentation of criterion 1 plus criteria 2 or 3
CT and MRI scan can be used in the diagnosis of sarcopenia to estimate muscle mass however the widespread use is hampered by the high cost and highly qualified personnel needed to do the interpretation. Both modalities are capable of detecting changes in muscle structure.
Although the time necessary for the image acquisition in the case of CT is shorter than for MRI, the radiation exposure is significant.
Dual-energy x-ray absorptiometry (DXA) is a well-established, low-radiation technique used to assess body composition and provides reproducible estimates of appendicular skeletal lean mass.1 Appendicular skeletal muscle mass (ASMM) is a measure of body muscle content, and it correlates with nutrition and physical status.
Bio-electrical impedance analysis (BIA) is a method which estimates the volume of fat and lean body mass based on the relationship between the volume of a conductor and its electrical resistance. The method is not expensive, requires no specialised staff and is relatively easy to use in clinical practice, both on ambulatory subjects or on hospitalised patients. Reference values have been established for older individuals.20
The Jamar dynamometer, or similar hydraulic dynamometer, is the gold standard for this measurement. However, for patients with advanced arthritis, the design of this dynamometer may be a limitation. A pneumatic dynamometer, such as the Martin vigorimeter, may be a good alternative. With this device, patients try to squeeze rubber balls (available in three sizes) with the same protocol as that used for the Jamar dynamometer. A variety of thresholds of grip strength have been proposed to characterize low muscle strength, ranging from 16 to 20kg for women and 26–30kg for men.
The second part of assessment depends on physical performance that will use two tests:
First is the Short Physical Performance Battery (SPPB) that evaluates balance, gait, strength and endurance by examining an individual’s ability to stand with the feet together in side-by-side, semi-tandem and tandem positions, time to walk 8ft and time to rise from a chair and return to the seated position five times.
The second test is Timed get-up-and-go test (TUG) which measures the time needed to complete a series of functionally important tasks. TUG requires the subject to stand up from a chair, walk a short distance, turn around, return and sit down again.
Inadequate protein intake can also contribute to sarcopenia and decreased function. A prospective cohort study found that adults aged 70 to 79 with protein intake ≤0.8 g/kg/day (the recommended dietary allowance were at greater risk of developing mobility limitations over six years of follow-up than those with protein intake ≥1.0 g/kg/day.21
Screening tools for malnutrition are intended for the quick identification of patients at risk of malnutrition, for more in-depth nutritional assessment, or for identifying patients at risk of developing sarcopenia or even increased risk of mortality. The combination of screening and assessing for malnutrition and sarcopenia is recommended to screen for the presence of malnutrition-sarcopenia syndrome in at-risk patient populations, particularly older adults in clinical settings. The common tools used are Mini Nutritional assessment-Short Form (MNA-SF) and Simplified Nutritional Appetite Questionnaire –SNAQ.
Vitamin D is associated with neuromuscular performance but results on the association of vitamin D levels with muscle strength and physical performance in the older persons are somehow discordant. Some studies show a significant association between low vitamin D levels and poor physical performance, assessed by handgrip strength and the short physical performance battery – a lower-extremity objective performance based evaluation tool, including raising five times from a chair, maintaining balance in three more challenging positions and the four-meter usual walking speed test.22
A randomised study on sedentary older men with a vitamin D 23
Additional studies are needed to clarify the effect of vitamin D supplementation on skeletal muscle and its optimal serum levels to maintain a good physical function in advanced age.
Low physical activity and sedentary lifestyle are main causes of sarcopenia, exercise is a primary strategy in the prevention and treatment of sarcopenia. Both aerobic training and resistance training can improve the rate of decline in muscle mass and strength with age.24
Aerobic exercise has beneficial impact on sarcopenia by improving skeletal muscle insulin sensitivity; stimulating skeletal muscle hypertrophy; and increasing skeletal muscle mass. Examples include treadmill, cycling, jogging, light swim etc.
In comparison to aerobic training, resistance training has a greater effect on increasing muscle mass and strength and attenuates the development of sarcopenia.24
Resistance training is a form of exercise in which muscle contracts against an external load. Equipment commonly used to perform resistance training includes free weights, exercise machines, body weight, and elastic bands.25 Examples include bicep curl, arm raise, tennis ball squeeze and lawn mower pull exercises for upper extremity strengthening and standing leg curl, hip extension, hip flexion, knee extension, side hip raise, and toe stand exercises for lower extremity strengthening performed at least one set of 8–12 repetitions.
Hypogonadism is one of the causes of sarcopenia. Testosterone is a steroid hormone produced by the Leydig cells of the testes.26 After the age of 30 years, testosterone levels decrease at a rate of 1% per year.27 Therefore up to 70% of men older than the age of 70 years, are likely to have reduced testosterone levels.28
Studies have shown a relationship between muscle mass and its function with testosterone.26 In a study by Baumgartner RN, et al. (1999), elderly men’s muscle mass was associated with serum free testosterone and insulin like growth factor 1 (IGF1).29 Another study shows that age related reduced testosterone levels is associated with reduced capacity of maximum voluntary neuromuscular performance in older people.30
Studies have shown that in humans, testosterone treatment increased type I and type II muscle fibers.31,32 This could be a potential drug treatment for sarcopenia, however its side effects of increased hematocrit levels and increased risk of cardiovascular disease is a concern.26
There are many medications in phase 1 or 2 trials for treatment of sarcopenia. These include activin receptor antagonist, myostatin or activin inhibitor, and selective androgen receptor modulator (SARM).
Dr Irfan Muneeb, Consultant Geriatrician
Dr Sakhawat Ali, Specialty Doctor, Medicine
Dr. Muhammad Josheel Naveed, Consultant Physician
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...