Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Back pain is a common symptom that can be the harbinger of serious disease, particularly in elderly patients. Separation of serious pathologies such as malignancy, infection, and cauda equina syndrome from benign axial back pain is a challenge. The red flags have clinical use for assisting in obtaining key features in the history and examination that may relate to sinister pathology. Knowing what and when to refer to a spinal specialist such as an orthopaedic surgeon or neurosurgeon is important. Cervical radiculopathy, myelopathy, and scoliosis may require specialist skills for discectomy, decompression, and reconstruction. This article deals with the assessment and treatment of cervical myelopathy and scoliosis.
Back pain is a common symptom that can be a harbinger of serious disease, particularly in elderly patients. The clinical dilemma is to separate the serious spinal disorders presenting as back pain or neurological symptoms from the benign axial back pain that affects a substantial proportion of the population at some point in their lives.1 The prevalence of back pain varies with age, with a point prevalence of 17–30%, a one-month prevalence of 19–43%, and lifetime prevalence of 60–80%.2
In a survey, 80% of people older than 60 years of age recalled an experience of back pain in their lifetime.2 Degenerative changes occur in almost all patients as part of normal ageing. At age 20 years, degenerative changes are noted on X-ray and MRI in less than 10% of the population.3 By age 40 years, such changes are seen in 50% of the asymptomatic population and by the age of 60, this number reaches 90%. This third article covers cervical myelopathy and scoliosis. The key points are shown in Box 1 and Figure 1 shows a normal MRI of the cervical spine.
Box 1: Key points
|
Using flags to identify patient-specific factors assists in the day-to-day management of spinal disorders. Red flags help to identify risk factors for serious spinal disorders (Box 2). Yellow flags help to define psychosocial obstacles to recovery. Blue flags are related to occupational factors. Black flags may be administrative obstacles to people returning to employment. Orange flags identify psychiatric disorders. In elderly patients, who are more likely to be retired, doctors should be aware of the red and yellow flags. Serious spinal disorders can be an important threat to life or to quality of life.
Box 2: Red flags for assessment of back pain4,5
|
Elderly people are at risk of falls. Cervical myelopathy contributes to this hazard. Spinal-cord compression can sometimes cause irreversible ischaemic changes such that the surgical treatment will have the limited objective of preventing further deterioration, rather than producing improvement. The long-tract signs and upper motor-neurone findings result from a reduction in the space available for the cervical spinal cord.6 The contributing degenerative processes are protruding intervertebral disc, deformed uncovertebral process, apophyseal joint arthritis and ossification of the posterior longitudinal and yellow ligaments.7 The reduction in the anteroposterior diameter of the spinal canal that occurs causes dynamic cord compression in flexion or extension, dynamic changes in the intrinsic morphology of the spinal cord, and alteration of its vascular supply.6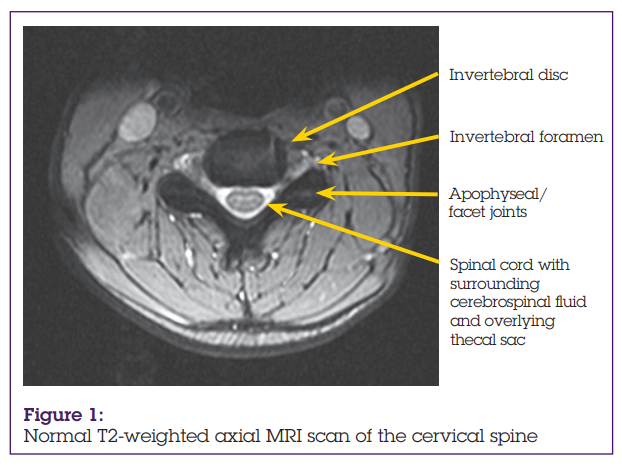
Absolute stenosis is defined by a canal measuring 10 mm in anterior-to-posterior dimension, and relative stenosis is a 13 mm canal.8 Both radicular and myelopathic complaints arise when the canal is narrowed to these critical dimensions because the cord itself occupies between 0·8 and 1·3 cm in the anterior-to-posterior dimension, and soft tissues take up another 2–3 mm.9 Further compromise of the already narrowed space (especially extension) increases the likelihood of incurring a clinically significant neurological deficit with even minor traumatic events.10 Direct mechanical trauma and indirect ischaemia contribute to mechanical dysfunction. Damage to grey and white matter associated with cord atrophy, demyelination, and infarction is often located several segments above or below the site of maximum cord compromise.11
Patients with cervical spine disorders most commonly complain of local and referred pain, headache, dizziness or disturbance of the equilibrium, paraesthesias, and weakness in the upper and lower limbs.12 In addition to a complete neurological assessment, including an examination of the cranial nerves as well as the legs and arms, laboratory investigations may be required.
The neurological examination aims to differentiate between nerve-root and spinal-cord compression. Neck pain can be the first clinical symptom of a slowly growing acoustic neuroma, with an absent corneal reflex being the first sign. Patients with referred pain in the region of the trigeminal nerve commonly present with underlying pathology in the upper cervical spine, often observed in atlanto-axial instability due to rheumatoid arthritis.13
Lhermitte’s sign—electrical pain along the spine radiating to the extremities during maximum flexion and extension of the cervical spine—is described in patients with multiple sclerosis as well as in spinal-cord compression.14 Radicular arm pain during side-bending rotation and manual compression of the head is Spurling’s test, and expresses itself as a motion-induced radicular irritation or compression, radiating pain along the involved dermatome.12
According to the type of lesion, the spinal cord will react primarily with demyelination of the descending or ascending pathways, or both, with the classic symptoms of tetraspasticity, pathologically increased muscle-tendon reflexes, positive Babinski sign, absent abdominal reflexes, and decreased sense of vibration in the lower extremities.12 Some patients with spinal-cord compression will present with atrophy of the small muscles of the hands, as a result of segmental necrosis of anterior horn cells.15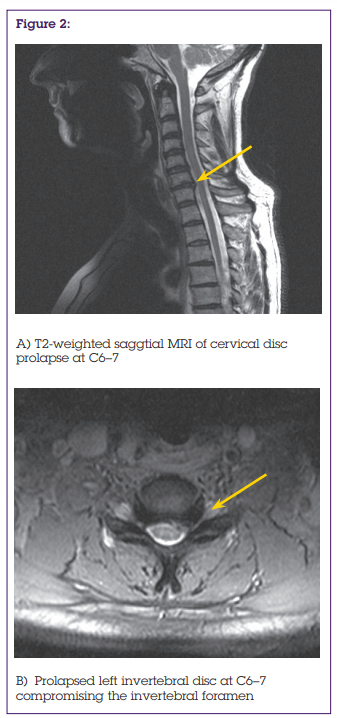
In the differential diagnosis of cervical spondylosis with involvement of neural structures leading to cervical spinal myelopathy, important considerations are peripheral neuropathic causes such as multiple sclerosis, amyotrophic lateral sclerosis, toxic-metabolic disorders (diabetes, alcoholism, vitamin B12 deficiency),16 or rheumatoid arthritis with cervical spine involvement, shoulder complaints, and finally psychogenic disorders.12 Blood tests to help with diagnosis include full blood count, urea, and electrolytes, inflammatory markers such as erythrocyte-sedimentation rate and C-reactive protein, vitamins D and B12, folate levels, and thyroid function. Imaging techniques include plain cervical spine X-rays, CT, and MRI.
Dynamic X-rays of the cervical spine help to define whether patients have sufficient lordosis to successfully undergo laminectomy for stenosis. On static or dynamic films, a minimum lordotic curvature of 10° is required if laminectomy is to be done, which allows the cord to migrate away from ventrally situated osteophytes or ossification of the posterior longitudinal ligament.17 Candidates for laminectomy or laminoplasty should also have less than 7 mm of ventral ossification of the posterior longitudinal ligament, or spondylosis.18 If laminoplasty is considered, a minimum of 14mm of anterior-posterior decompression should be feasible for those with spondylotic myelopathy, compared with a greater 17 mm for those with ossification of the posterior longitudinal ligament.19 Frank instability is defined on flexion and extension studies by more than 3·5 mm of subluxation, greater than 20° of angulation, and greater than 1–2 mm of motion demonstrated between the tips of adjacent spinous processes.12
MRI in multiple planes (figures 2 and 3) readily defines spinal-cord and nerve-root compression as well as other intrinsic cord abnormalities.6 Cerebrospinal fluid remains hypointense on T1-weighted studies, and the cord appears isointense. T2-weighted studies create a myelographic image because cerebrospinal fluid becomes hyperintense, and the cord itself stays hypointense. Increased cord signals on T2 images suggest demyelination. Oedema or myelomalacia are poorer prognostic findings for patients with spondylotic myelopathy compared with those exhibiting ossification of the posterior longitudinal ligament.20 Patients with severe, irretrievable cord damage should not be considered as surgical candidates because their chances of recovery are very small.21
Neurophysiologically, somatosensory-evoked potentials and motor-evoked potentials are most helpful in the investigation of the central nervous pathway; electromyography is more useful for evaluation of the peripheral segments of the sensory and motor pathways.12 The European Myelopathy Score is used to assess the severity of cervical myelopathy.22 It has five subscores: gait (5 points), bladder and bowel function (3 points), lower motor-neurone function (4 points), proprioception and coordination (3 points), and sensory disturbance (3 points). The maximum number of points a patient can have is 18. This score helps doctors to judge the natural course of disease and to determine the timing of surgery. It also allows objective control of post-operative outcome. The minimum score is 5, and the score classifies cervical myelopathy into 3 grades: grade III (5–8 points); grade II (9–12 points); and grade I (13–16 points). People scoring 17 or 18 points are considered free of signs of cervical myelopathy.
Conservative management of mild cervical stenosis or even more severe cervical stenosis in elderly people, who are not surgical candidates includes cervical collars, short-term steroidal and long-term non-steroidal anti-inflammatory medications, physical therapy, biofeedback techniques, and occasional epidural steroid injections.23 Occasionally, patients with mild myelopathy, despite MRI scans showing increased cord signals, can be managed successfully with various traction methods and cervical bracing techniques.24
Box 3: Main types of scoliosisType 1: Primary degenerative scoliosis (de novo form) This scoliosis is mostly located in the thoracolumbar or lumbar spine.26 It is basically the result of an asymmetrical degenerative change of the disc with the consecutive development of a frontal deviation and concomitant rotation with the facet joints on one side as a pivot.27 The apex of this curve is usually between L3 and L4 or L2 and L3, or second most frequently between L1 and L2. This type of scoliosis consists of a frontal and a sagittal deviation in the form of mostly a flat back or lumbar kyphosis.26 The sagittal malalignment is usually responsible for the severe postural back pain of the patients.27 Spinal stenosis is more often seen in primary degenerative scoliosis than in secondary degenerated idiopathic curves.28 The disc degeneration ends up with spondylosis, disc bulging, osteophytes, and facet joint arthritis with hypertrophic capsules, ligamentum flavum, and calcification of these structures with osteophytes, all on the costs of space in the spinal canal and foramina, thus contributing to the formation of spinal stenosis.27 Type 2: Progressive idiopathic scoliosis Occurs in adult life, affecting the thoracic or lumbar spine, or both.29 The degenerated idiopathic scoliosis, mostly in the lumbar or thoracolumbar spine is quite frequently combined with spinal stenosis at a relatively young age (late adolescence to about 40 years), specifically in the adjacent lower segment after surgical instrumentation.27 Type 3: Secondary degenerative scoliosis 3a) Scoliosis subsequent to idiopathic or other forms of scoliosis, or occurring in the context of a pelvic obliquity due to a discrepancy in leg length, hip pathology, or a lumbosacral transitional anomaly, mostly located in the thoracolumbar, lumbar, or lumbosacral spine.30 3b) Scoliosis secondary to metabolic bone disease (mostly osteoporosis) combined with asymmetrical arthritic disease or vertebral fractures, or both.31 |
Scoliosis is a deformity of the normal vertebral alignment of the spinal segments and occurs in both the coronal and sagittal planes.1 Scoliosis is diagnosed in adult patients when it occurs or becomes relevant after skeletal maturity, with a Cobb angle of more than 10° in the coronal plane.25 Box 3 describes the four main types of scoliosis.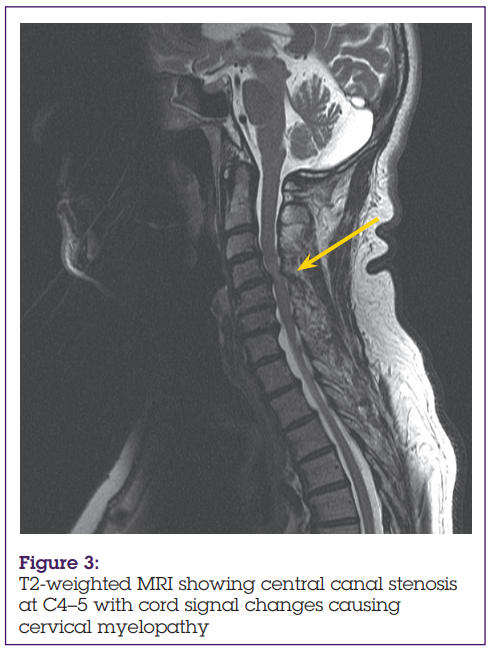
In elderly patients, scoliosis can be aggravated by osteoporosis.30 The potential for individual asymmetrical deformation and collapse in the weak osteoporotic vertebrae is increased and contributes further to curve progression.27 The destruction of discs, facet joints and joint capsules usually ends in some form of uni-segmental, multi-segmental, frontal latent, or obvious instability. Patients might not only have a spondylolisthesis (slip in the sagittal plane) but also translational dislocations in the frontal plane.25 The biological reaction of an unstable segment in the spine is the formation of osteophytes at the facet joints (spondyloarthritis) and at the vertebral end plates (spondylosis) both contributing to increasing narrowing of the spinal canal together with the hypertrophy and calcification of the ligamentum flavum and joint capsules, creating central and recessal spinal stenosis.32
The most frequent clinical problem of scoliosis is back pain situated either at the apex of a curve or in its concavity, and facet joint pain can be localised in the countercurve from below the curve to above the curve.27 The pain could be combined with radicular leg pain, or can be an expression of muscular fatigability, or of real mechanical instability. It can be constant and non-specific, or present only on standing or sitting, or during certain activities or movements; pointing to a mechanically unstable segment or a whole spinal region.
Patients with scoliosis also complain of radicular pain and symptoms of claudication when standing or walking.33 Root compressions due to spinal stenosis can occur at the bottom of the curve or at the transition to the sacrum and can be linked to a hypermobility of an overloaded bottom segment, especially with stiff curves. Red flags in scoliosis include back pain, limb weakness, sensory disturbance, abnormal gait, and a left-sided curve. These signs warrant a complete neurological exam and further imaging studies.
A real neurological deficit may also be the reason for presentation. Individual roots, several roots, or the whole cauda equina may be involved with apparent bowel and bladder problems. This is rare and when present, is due to significantly compromised space in the spinal canal with acute aggravation and decompensation. The final consideration on presentation is curve progression, which may occasionally indicate surgical intervention to avoid further degeneration and progression in a patient with potential medical risks, including respiratory and neurological compromise.
Suitable investigations include plain X-rays with dynamic views of the spinal segments involved. A spiral CT is very useful for rapid vertical reconstruction of the spine and, in conjunction with a myelogram, obtaining a clear understanding of the pathogenesis.29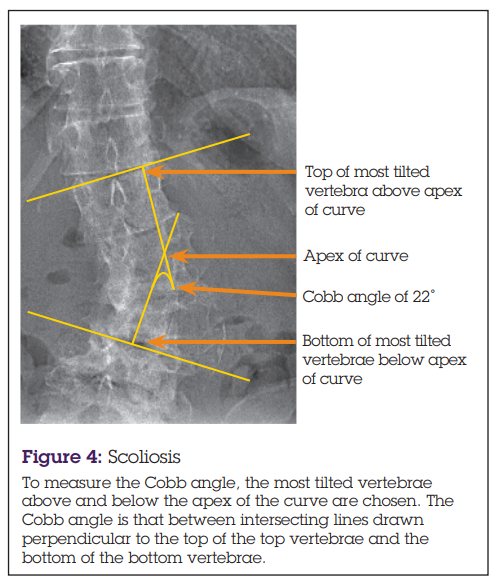
The non-surgical treatment measures for scoliosis include non-steroidal anti-inflammatory drugs, muscle relaxants, pain medication such as paracetamol and opiates, and neuropathic agents such as amitriptyline and gabapentin. Non-drug treatments include muscle exercises, swimming, gentle traction, and use of a well fitted brace to support the painful area.34,35 Selective nerve-root blocks and therapeutic epidurals may also be of benefit. The decision for surgical management is influenced by the patient’s general health, age, condition of bone quality, and the patient’s expectations.31 The surgical concepts include decompression procedures, stabilisation and fusion procedures, and correction procedures, which can be done separately or together, depending on the patient’s overall symptoms.27
Osteoporosis is a major concern in the treatment of adult scoliosis.27 Most elderly patients with degenerative scoliosis are female and during menopause, they may have increasingly symptomatic scoliosis due to curve progression as an asymptomatic load makes weakened vertebrae more wedged and deformed. Surgical treatment is complicated by the weak bone because implants are more difficult to be anchored and fixed; making the instrumented fusion prone to complications.27 Large diameter screws and adapted threads to improve bone purchase as well as cement re-enforcement of the screw’s anchorage have also been proposed to help with these difficulties.36,37
The authors declare no conflict of interest.
Mr Tosan Okoro, Clinical Research Fellow, Leicester General Hospital, University Hospitals Leicester NHS Trust, Gwendolen Road, Leicester LE5 4PW, UK. Email: [email protected]
Mr Phillip Sell, Consultant Orthopaedic Surgeon, Leicester General Hospital, University Hospitals Leicester NHS Trust, Gwendolen Road, Leicester LE5 4PW, UK.
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...