Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


On Saturday (22nd May), Public Health England released a report presenting the data on the new Covid variant: B.1.617.2.
This new variant of concern, which is known as the Indian variant, is thought to be as much as 50% more infectious than the B.1.1.7 (Kent) variant, which saw the UK dive back into a nationwide lockdown in November 2020.
However, in a recent press release, the Government assured the general public that the AstraZeneca and Pfizer vaccines are both “highly effective” against the new variant after two doses.
The study revealed that the Pfizer-BioNTech vaccine was 88% effective against symptomatic disease from the B.1.617.2 variant two weeks after the second dose, while the AstraZeneca vaccine was 60% effective after the same period. This compares to 93% (Pfizer) and 66% (AstraZeneca) effectiveness against the Kent variant.
The government say the difference in effectiveness between the vaccines is thought to be because the rollout of the second doses of AstraZeneca was later than for the Pfizer vaccine. Other data suggests that it takes longer for the AstraZeneca vaccine to reach maximum effectiveness.
Both vaccines were 33% effective against symptomatic disease from the B.1.617.2 variant, three weeks after the first dose compared to around 50% effectiveness against the B.1.1.7 variant.
The Health Secretary, Matt Hancock, described the new evidence as “ground breaking”, while the minister for Covid-19 Vaccine Deployment, Nadhim Zahawi, said the data was “astounding.”
However, others believe there is cause for concern, after PHE updated their risk assessment from amber to red in areas including transmissibility between humans and vaccine effectiveness.
Anthony Costello, professor of global health at University College London, tweeted expressing his concerns about the further easing of lockdown rules on the 21st June. He said: “This is a travesty of the data in the PHE report sneaked out late last night with a misleading press release.”
Experts are concerned that both vaccines are only 33% effective three weeks after the first dose. This means that those who have only had one dose, are not very well protected from the virus.
In the UK, you have to wait 12 weeks between your first and second dose if you’re under 50, while those over 50 must wait 8 weeks.
While it is welcome news that the vaccines are highly effective for those who have had both doses, currently only 34% of the population are fully vaccinated. This means the remaining two thirds of the population are very much at risk of being exposed to the virus.
There is even concern for those who are fully vaccinated, as scientists do not know how long immune protection lasts. This means that those who had their first dose right at the beginning of the vaccination programme in December 2020 and January 2021 could soon be left vulnerable again. This group is of particular concern as it is made up of the most vulnerable and elderly in society.
There is however a study trialling a third dose of the Covid vaccines to find out if another jab could provide added protection from variants of concern and to decipher which vaccine is the most effective.
The data suggests high levels of transmissibility, with the estimated growth advantage of Indian variant at 99% a week, which is twice as fast as the Kent variant. The Indian variant also has a higher secondary attack rate than the Kent variant, which means it is more likely to infect close contact of an infected person.
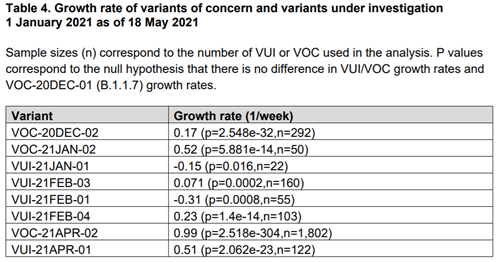
Taking this data into account, the PHE concluded that it is “realistically possible that this new variant of concern could be 50% more transmissible”, aligning their views with SAGE.
The good news is that although there are particularly high cases in the North West of England (1,122 cases), growth is not happening everywhere. In London, although there are 650 cases of the new variant, they haven’t increased much over the past two weeks. There is also no evidence that the Indian variant causes more severe illness than any other variant.
The government has also come under fire for reportedly putting pressure on PHE to exclude crucial data on the Indian variant in schools. The Observer reported that a pre-print of the PHE report included a page of data on the spread of the new variant in schools, yet the page was removed in the final copy of the report.
In hotspots such as Bolton, cases involving the variant are rising fastest among school-age children, the Guardian says. Information accessed by the Observer found that 164 cases of the new variant were linked to schools up to 12 May, or 7.8% of a total of 2,111 cases. Since then, the number of total cases has increased by 62%, to 3,424 cases.
This data has still not been published, despite calls from union officials and scientists who say teachers and families are being put at risk, particularly as children are no longer required to wear facemasks while at school. PHE say the data will be published in “due course”.
It is important to remember that the picture we are looking at is now out of date. All the data which has now been analysed has been taken from a period before the 17th May, when the lockdown restrictions eased further and allowed for socialising indoors as well as outdoors.
In order to get a good idea of how the easing of restrictions has affected case numbers, we will have to wait a few weeks. At which point, experts fear, it could be too late.
Even so, the Health Secretary has expressed his confidence in the UK’s vaccination programme. Mr Hancock said: “I’m increasingly confident we’re on track for the roadmap because this data shows the vaccine after two doses works just as effectively, and we all know that the vaccine is our way out of this.”
However, others disagree. Professor Christina Pagel says the data does not support moving to step four of the roadmap unless the current risk reduces significantly. She tweeted: “Right now, we should reintroduce masks in schools, accelerate [vaccinations] and make [vaccinations] more accessible to communities, support people to isolate and support businesses [and] schools to improve ventilation.
“If B.1.617.2 does not start looking less scary, we must wait until we have fully [vaccinated] more people. If cases keep going up next week – consistent with continued rapid growth of B.1.617.2 – we should consider rolling back step 3 of roadmap.
“Waiting too long as we did in March, September [and] December means that restrictions if they do come will be longer and harsher. We don’t want to do that AGAIN. As JUNIPER said for SAGE: ‘Incontrovertible evidence that B.1.617.2 is more transmissible may come too late’”.
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...