Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Medical literature has been awash with information about the cutaneous manifestations of Covid-19. What is interesting is that although Covid-19 shares 79% of its genetic makeup with the original severe acute respiratory syndrome (SARS), and about 50% with the Middle East respiratory syndrome coronavirus (MERS), there is no evidence that either SARS or MERS caused cutaneous symptoms.1 Therefore, are cutaneous changes something specific to Covid-19?
Reports of cutaneous manifestations of Covid-19 were first reported in the original cohort of patients from Wuhan which showed that among 1,099 patients, only 2% reported a rash.2
With national lockdowns in many countries resulting in the cessation of routine secondary care services, many hospital specialists were re-deployed to the front line services and this is when dermatologists started to notice skin problems associated with Covid-19. The first report in March 2020 came in a letter to the Journal of the European Academy of Dermatology and Venereology from Italian dermatologists, speculating that skin manifestations of Covid-19 were similar to the cutaneous involvement observed with common viral infections.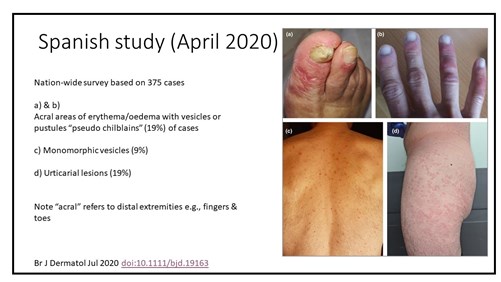
Unfortunately, no one took any pictures because of the potential yet unknown, risk of infecting other patients by introducing a photographic device in a restricted room.3
From the collected data of 88 patients, 18 patients (20.4%) developed cutaneous manifestations. Eight patients developed cutaneous involvement at the onset and 10 patients after hospitalisation.
Cutaneous manifestations recorded were an erythematous rash (14 patients), widespread urticaria (three patients) and chickenpox‐like vesicles (one patient), all mainly on the trunk. Itching was low or absent and usually lesions healed in few days. The dermatologists concluded that there was not any correlation with disease severity.
The next piece of evidence came from a Spanish study a month later. It found 375 cases of Covid-19 skin manifestations and highlighted five clinical patterns associated with different patient demographics, timing and prognosis. The lesions were classified as acral areas of erythema with vesicles or pustules (pseudo-chilblain) (19%), other vesicular eruptions (9%), urticarial lesions (19%), maculopapular eruptions (47%) and livedo or necrosis (6%).4
The study gave some insight into the relationship between the onset of clinical symptoms and the onset of rash. Vesicular eruptions appeared early in the course of the disease (15% before other symptoms). The pseudo-chilblain pattern frequently appeared late in the evolution of the Covid-19 disease (59% after other symptoms), while the rest tended to appear with other symptoms of Covid-19. People also began to report skin problems to the Covid-19 Symptom Study App created by Professor Tim Spector and colleagues at King’s College London.5 Among 336,000 self-reports, 8.8% of people who tested positive for Covid-19 had a rash versus 5.4% who were negative. Among 12,000 with skin rashes and who were Covid-positive, 17% had rash as the first symptom and for 21% rash was the only symptom.
People also began to report skin problems to the Covid-19 Symptom Study App created by Professor Tim Spector and colleagues at King’s College London.5 Among 336,000 self-reports, 8.8% of people who tested positive for Covid-19 had a rash versus 5.4% who were negative. Among 12,000 with skin rashes and who were Covid-positive, 17% had rash as the first symptom and for 21% rash was the only symptom.
One interesting skin condition reported as a symptom of Covid-19 is pseudo-chilblains. The prefix “pseudo” was applied because chilblains normally occur during colder weather and these lesions were seen in more a temperate climate. The pseudo-chilblains were commonly seen in children and adolescents and caused pain and an intense burning sensation. They also tend to be associated with more mild disease. In one study, 55% had these lesions as the only symptom of Covid-19.6 However, whether pseudo-chilblains were actually caused by Covid-19 was a matter of debate with three studies (see below) all concluding that there was no causal relationship:
In contrast, it has been suggested that pyrexia with urticaria is suggestive of Covid-19.
The least common skin reaction (circa 6%) is livedoid reaction. Under normal circumstances, causes include blood vessel spasm, abnormal circulation near skin surface and cold weather.
A case report in the British Medical Journal also described a 12-year-old boy with a two-week history of a generalised maculopapular exanthem on the trunk, arms and legs four weeks after a full recovery from Covid-19.10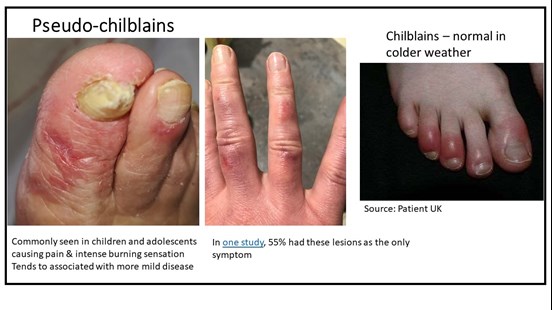 No specific treatment guidance has been issued for Covid-19 skin conditions. One case of Covid toe (pseudo-chilblains) reported in Dermatology Nursing Journal suggested treatment was to keep toes warm (double socks/foot warmers) and evidence suggests it resolves within one to two weeks, but can take up to eight weeks. Emollients can be used for pruritic eruptions.
No specific treatment guidance has been issued for Covid-19 skin conditions. One case of Covid toe (pseudo-chilblains) reported in Dermatology Nursing Journal suggested treatment was to keep toes warm (double socks/foot warmers) and evidence suggests it resolves within one to two weeks, but can take up to eight weeks. Emollients can be used for pruritic eruptions.
To conclude, several different cutaneous manifestations appear to be related to infection with Covid-19. The question is: are they an immune reaction to viral nucleotides (viral exanthem), secondary consequences of infection, or are they symptoms due to adverse reactions of the drugs used to treat the condition itself?
This article is based on a GM webinar held in February 2021. The recording can be accessed at www.gmjournal.co.uk
Dr Rod Tucker is a Pharmacist researcher with an interest in dermatology
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...