Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Erectile dysfunction can be an embarrassing topic, even though one-third of men might be diagnosed with some form of ED in their lifetime.
Every GP is familiar with the unhappy experience of talking to patients about erectile dysfunction (ED). It is easy to recall the awkward way many students would hesitantly broach the topic, asking the question too indirectly or circumspectly. And for many doctors in practice, the issue of how best to address erectile dysfunction with patients is never really resolved, remaining a matter best avoided by both parties.
To compound the problem, as GPs we know that there are multiple causes of erectile dysfunction, most commonly diabetes, cardiovascular disease, and anxiety. Yet many patients go on to be prescribed Viagra or a similar drug, or acquire it through some other route, with no further investigation of the underlying cause or causes of the dysfunction.
How can we do better? A useful starting point when managing patients with ED is to think of the penis as a barometer of health. With the general acceptance of a 3-year period1 between the onset of erectile dysfunction and significant risk of a cardiovascular event, addressing the problem early in the course of the disease can offer the opportunity for risk mitigation and disease reversal.1 Accordingly, when treating erectile dysfunction, an holistic approach (looking at cardiovascular health, hormone levels, lifestyle and risk factors, and mental health), and not just symptom management, is the best way to achieve a long term reduction in symptoms and an overall improvement in health. With this goal in mind, this paper summarises the epidemiology and physiology of ED, its risk factors, and its investigation and treatment.
Estimates of ED prevalence vary widely according to the choice of study methodology or demographics, but, in general, it is accepted that ED will affect around one-third of men at some point in their lives.2 Thus, Kubin et al.3 suggested that 5–20% of all men have moderate-to-severe ED, and though this proportion may seem surprising, several other studies have indicated similarly high levels. Braun et al.4 found, in a sample of over 4,000 men, an ED prevalence of 19%. Even higher levels were reported in the Massachusetts Male Aging Study, suggesting a prevalence of 52% ED in 1,700 men aged 40-70 years.5
Where age-stratified data are available, epidemiological studies generally point to the increasing prevalence of ED with age. The National Health and Social Life Survey (NHSLS) found that in a sample of 1,410 men the ED prevalence was 7% at 18-29 years, 9% at 30-39, 11% at 40-49, and 18% at 50-59.6 Underlying this pattern, most studies conclude that psychological issues usually explain ED in younger patients and that organic causes become more important with increasing years, an expected finding given the pattern of onset and progression of co-morbidities and chronic health conditions with age.
The process of erection is a complex neurovascular event, combining emotional, neurovascular, and hormonal responses. Disrupting any of these processes can result in ED.
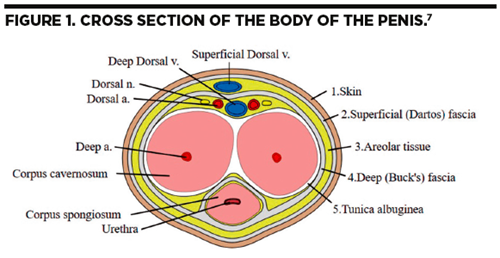
The penis itself is made up of several different discrete compartments, in particular, the corpus spongiosum, and corpora cavernosa (see Figure 1), and the glans (head of the penis). It is the cavernosa, in particular, the cavernous smooth musculature and the smooth muscles of the arteriolar and arterial walls that play a key role in erection.8 Even in the flaccid state, the penis is in a moderate degree of contraction, as often evidenced by the shrinkage than can occur in cold weather or stress responses. Sexual stimulation releases neurotransmitters from the cavernous nerve terminals, relaxing the cavernosa smooth muscles, and initiating a series of processes that result in a full erection.
 In more detail, the steps in this pathway are as follows:
In more detail, the steps in this pathway are as follows:
In addition to the vascular mechanisms, the autonomic, somatic, and peripheral nerves have a crucial role in the erectile process, and like the vascular component are just as vulnerable to disease. The hormonal influence on erectile dysfunction has come under particular scrutiny as there has been some debate around the overall of influence of testosterone on ED.9 Hypogonadism is a relatively common finding in patients with ED. Clearly androgens influence the growth and development of the male reproductive tract and secondary sex characteristics, and a lack of testosterone has been shown to reduce sexual interest, nocturnal erections, and the frequency of sexual acts.8 In particular, a chronic deficiency in testosterone has been shown in animal models to decrease penile arterial flow, induce venous leakage, and reduce about half of the erectile response to stimulation of the cavernous nerve.10,11
Due to the complexity of the erection mechanism, there are many ways to classify its pathophysiology, but it can be broadly described as organic, psychogenic, or a mixture of both. The International Society for Impotence Research (ISIR) offers one of the simplest methods of classification.12
Organic
Vasculogenic
Neurogenic
Arteriogenic
Anatomical
Cavernosal
Endocrinological
Mixed
Psychogenic
Generalised
Situational
While it is interesting to have this classification, the undifferentiated class of mixed organic and psychological causes represents a huge proportion of ED patients, and it is helpful to highlight some of the more common contributory factors. The risk profile commonly follows a pattern similar to that for metabolic syndromes or cardiovascular disease.
Johannes et al.13 found that diabetes mellitus was the most important risk factor for developing ED, owing to its effects on microvascular, macrovascular and neuropathic function, all of which influence the erectile process. Cardiac disease was the second biggest contributor to ED, even though ED itself may precede symptomatic cardiac disease by at least 3 years. Because endothelial dysfunction is common in both ED and cardiovascular disease, lifestyle factors such as smoking, obesity, inactivity, and chronic alcohol use were also identified as major contributors to erectile dysfunction. Alcohol use, or misuse, has a special place in ED. Although it is used routinely to reduce inhibition and anxiety about sexual performance, up to 72% of patients with chronic alcoholism have been reported as suffering some degree of sexual dysfunction.14
In addition to lifestyle factors, and metabolic and cardiovascular contributors to ED, the other significant organic cause of ED is low testosterone. In patients diagnosed with testosterone deficiency, there is an established association with the development of ED, as well as an increased risk of cardiovascular disease, muscle wasting, low mood, and decreased libido. In its contribution to ED, testosterone deficiency acts through multiple pathways.
Due to the complexity of the erection mechanism, there are many ways to classify its pathophysiology
Drugs that affect testosterone production, including many prescribed medications and recreational drugs, can therefore contribute to ED. For example, thiazide diuretics, antidepressants (SSRIs), antipsychotics or neuroleptics, corticosteroids, opiates, antifungals, certain antacids, and a variety of recreational drugs including cocaine, heroin, marijuana, methadone, anabolic steroids, and alcohol can all result in a reduction in useable testosterone.15 Where possible, therefore, medications that reduce testosterone levels or have an impact on ED should be reduced or changed. However, in those patients where chronic illness means a reduction or change in testosterone suppressing medication is not possible, further discussion with a specialist is advised to explore alternative treatment options.
Finally, cancer therapy is also often associated with ED, either as a direct result of surgical or radiotherapy treatment, especially in prostate cancer, or from chemotherapy disrupting the production of testosterone.
For patients with suspected ED, it is important to take a detailed sexual history, as well as recording any co-morbid medical, psychiatric, or surgical factors. Asking about sexual desire, relationship status, or even issues around sexual orientation and gender identity may help reveal an underlying psychological cause for ED. Differentiating between organic and psychological factors is essential in effective long-term management.
In detailed assessments of erectile dysfunction, the International Index of Erectile Function (IIEF) is a 15-point questionnaire that looks at sexual activity, sexual intercourse, sexual stimulation, ejaculation, and orgasm.16 In practice, it is unlikely that many GPs will use this scoring system owing to the time required, but abbreviated ED questionnaires are available, such as the Sexual Health Inventory For Men (SHIM).17
Where appropriate, physical examination for ED can be helpful in eliminating or confirming a diagnosis of trauma, Peyronie’s disease, or hypogonadal conditions. In addition, blood pressure, heart rate, and weight may be informative when considering metabolic or cardiovascular causes. A digital rectal exam of the prostate is not essential but may be relevant in patients with coexisting genito-urinary symptoms.
Because of the multifactorial causation of erectile dysfunction, the British Society of Sexual Medicine (BSSM) recommends a focused investigation based on the individual circumstances of the patient.18 If low testosterone is suspected as a likely cause of ED, a blood test for total testosterone should be taken before 11am. This is because testosterone naturally peaks in the early hours of the morning, and bloods taken after this time are likely to show a physiological decline in levels through the day. In patients where total testosterone is normal, but there is a high suspicion of testosterone deficiency, further testing to look at free testosterone is advised.15 In patients with confirmed low total testosterone, or low free testosterone, further investigations are often needed, including FSH, LH, and prolactin levels, to ascertain if the cause is primary or secondary hypogonadism.
Other common tests in ED include HbA1c (or appropriate diabetic screening), and cholesterol to assess cardiac risk. In patients with confirmed ED but with an unclear cause, other tests to consider in primary care include TSH, oestradiol, liver function, renal function, and full blood counts, as all can contribute to ED through various pathways. It is often worth checking TSH levels because ED is also associated with both hyper- and hypothyroidism. Hyperthyroidism can result in increased circulating oestrogen levels, and therefore a diminished libido. Hypothyroidism can result in low testosterone production and elevated prolactin levels, both of which contribute to ED.8
Effective and long-term treatment of ED should be holistic. Although phosphodiesterase type 5 (PDE5) inhibitors play a crucial role in the management of ED, as explained shortly, they are not a universal solution. Rather, treatment should be based on three core considerations:
The most common form of therapy for ED remains the use of oral PDE5 inhibitors. The molecular mechanism of penile smooth muscle relaxation is complex, but essentially sildenafil inhibits the action of PDE5, which results in increases in intracellular concentrations of cGMP, and allows for greater blood flow to the penis and smooth muscle relaxation.19 The success rate of PDE5 inhibitors has been estimated at 60-70%.20
When prescribing PDE5 inhibitors, it is important to educate patients on the mechanism of action of the drugs, especially due to the fact that they do not result in an immediate erection, and that they do not cause an erection without sexual stimulation. One of the most common problems with ED treatments is matching patient expectations with what the treatments can actually achieve.
In general, there are 4 PDE5 inhibitors available in the UK:
Unlike many other forms of ED treatment, ESWT appears to have very few side effects
In patients where PDE5 inhibitors are either not desired, or contraindicated, vacuum erection devices can be effective. Satisfaction rates range from 35-84%.18 The most common side effects of vacuum devices include bruising, local pain, and failure to ejaculate. Partners sometimes report the penis feels cold. Despite its relative success rate, vacuum devices are not commonly considered for treatment for ED in primary care.
In patients where PDE5 inhibitors and vacuum devices fail, referral to specialist clinics provide other therapeutic options such as the prostaglandin vasodilator alprostadil, administered either by injection or urethrally. Alprostadil acts directly on the penile and vascular smooth muscle cells to stimulate the production of cyclic AMP. Unlike PDE5 inhibitors, aprostadil does not require nitric oxide, or even an intact nervous system.24 Where prostaglandin vasodilators are either contraindicated, or fail to work, other specialist urological treatments include penile prosthetics, either malleable or inflatable. Obviously, these treatments are reserved for a very small proportion of ED patients.
Finally, it is worth noting the recent introduction of extracorporeal shock wave therapy (ESWT) for ED. This therapy is designed to cause neovascularization to areas of the penis with poor blood flow.25 Unlike many other forms of ED treatment, ESWT appears to have very few side effects. A systematic review and meta-analysis performed by Clavijo et al. in 201726 found that ED treatment with ESWT resulted in significant increases in patients improved Index of Erectile Function scores. Unfortunately, only 602 patients were analysed, and although the evidence for ESWT is promising, more information is needed to help target the therapy to the most appropriate ED patients.
Erectile dysfunction limits the quality of life for millions of men. Yet its significance goes beyond successful sexual function. By addressing the issue earlier rather than later with patients, GPs can mitigate the physical and psychological impact of ED, as well as reducing future health risks and potential complications.
Dr Jeff Foster
GP with an interest in Men’s Health
www.drjefffoster.co.uk
Private/NHS GP, West Midlands
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...
