Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Medication errors are a significant cause of iatrogenic morbidity in the inpatient setting. An estimated 4-15% of UK inpatients suffer an adverse drug reaction (ADR) during their hospital stay.
Medication errors are a significant cause of iatrogenic morbidity in the inpatient setting. An
estimated 4–15% of UK inpatients suffer an adverse drug reaction (ADR) during their hospital
stay.1-3 A large proportion of ADRs result from medication errors, which are by definition
preventable.
This article reviews drugs and their “DAINGER” profile with the aim of improving
the quality of the documentation of drug prescribing on neurology and neurorehabilitation wards.
The term ‘medication error’ may refer to dispensing or prescribing errors. Common reasons for prescribing errors include a lack of information about the patient, poor knowledge of the drug in question, and other factors such as stress, tirednesss and ward distractions.4-6
The quality and detail of the documentation of newly prescribed drugs in the patient’s notes has been neglected in previous studies. However a number of studies have investigated methods for improving the contemporaneous documentation of prescriptions in patients’ notes. In one study serial audits over nine years found that education sessions improved the detail of the documentation of prescriptions.7
Other studies have investigated the use of sticker-based interventions and acronyms in relation to prescribing. A simple pre-printed sticker intervention improved compliance with the antibiotic prophylaxis policy in one hospital by acting as a visual reminder to doctors.8 In several studies, the acronymic prescribing tool ‘NO TEARS’ was found to be an invaluable aide memoire for GPs when performing a review of a patient’s medications.9
Based on the evidence in the existing literature, the DAINGER profile was created. This is an acronymic case note-based trigger tool, designed to improve the quality of both prescribing and its documentation in hospital notes. Its aim is to help medical staff structure their thinking for a specific drug and reduce ADRs caused by prescribing errors.
The acronym provides a series of prompts that help the prescriber, before they put pen to prescribing chart, to consider some important issues regarding the drug in question (Box 1).
Box 1: Questions raised by the letters of the word DAINGER
| DAINGER profile |
| D Dose of the drug |
| Daily number of times that the drug is given |
| Delivery (administration) |
| Diagnosis for which the drug is given |
| A Adverse drug reactions that the drug can cause |
| I Interactions of the drug with other drugs |
| N Non-pharmacological alternatives considered |
| G Guidelines followed (such as NICE guidelines) |
| E Explained to the patient and family where appropriate |
| R Review date |
From the hospital notes a retrospective audit of the documentation relating to 224 new prescriptions over a 16- month period was performed. Data was obtained from both the patient notes and the drug charts on three selected neurological wards at University Hospital Wales (UHW), Cardiff and Rookwood Hospital, Cardiff.
The quality of documentation in the hospital notes at or around the time at which drugs were prescribed (according to the drug charts), was judged according to the components of the DAINGER profile. This provided retrospective data.
A prospective audit was then initiated following the introduction on to the hospital wards of stickers, suitable for placement and use in the hospital notes, on which the DAINGER profile acronym was printed with enough space for the hospital doctors to document relevant information for each category of the profile.
A meeting with the prescribing doctors on the wards was conducted. The importance of ADRs was explained to the medical staff and they were asked to participate in the study by completing a DAINGER sticker for each drug they prescribed, at the time of prescribing, and then include it as part of that day’s entry in the hospital notes. Over a period of five weeks, data on the documentation of 117 newly prescribed drugs was collected from the three wards.
The results showed a statistically significant improvement associated with the use of the DAINGER profile stickers.
At UHW the mean percentage of categories about which there was some documentation in the notes was 1.09% retrospectively and 18.65% prospectively (p<0.0001), and in Rookwood 3.23% and 32.44% (p=0.002).
Prospectively (UHW and Rookwood combined) 25% of the prescriptions had something documented under the 10 categories of the DAINGER profile whereas this was only 2% retrospectively. The improvement was statistically significant for every DAINGER category recorded and statistically significant for the mean of all the categories (p-values < 0.05).
Box 2: The comparison between retrospective and prospective data for each category of the DAINGER profile
| Dose | 2.7 | 29.1 |
| Daily number of doses | 0.9 | 29.1 |
| Delivery route | 3.1 | 29.9 |
| Diagnosis | 6.7 | 31.6 |
| ADRs | 0.4 | 18.8 |
| Interactions | 0.9 | 19.7 |
| Non-pharmacological alternatives | 0.0 | 17.9 |
| Guidelines | 0.4 | 23.1 |
| Explained to patient | 0.4 2 | 5.6 |
| Review date | 1.3 | 27.4 |
| MEAN | 2 | 25 |
The results show that the use and completion of DAINGER profile stickers at the time of prescribing significantly improves the quality of the documentation in the hospital notes.
In spite of drastic improvements in terms of percentages, a large proportion of drugs were still not documented. On average, 75% of drugs were still not documented after the stickers were introduced. The incomplete concordance is complicated and multi-factorial, however on the basis of our time on the wards we think it could be explained in relation to three broad categories.
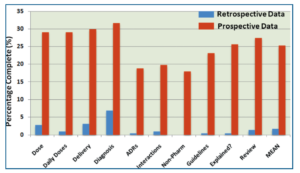
Figure 1. Percentage of medical notes in which information was complete for the different components of the DAINGER profile; retrospective and prospective study in columns one and two respectively
Doctors on-call at weekends were unaware of the existence of the stickers. As a large number of drugs were prescribed by these doctors, it accounts for the majority of the non-concordance.
The probability of doctors making prescribing errors increase when they are hungry, physically or mentally tired.9 In the context of this study, at times when the ward was exceptionally busy, it is likely that the doctors perceived other pieces of work to be of higher priority than detailed documentation.
It is feasible that apathy could play a part in the minds of some individuals, or even ‘resistance’ to a new system that they perceive to be of no immediate or long-term benefit in a clinical situation.
It is important that doctors throughout all specialties are educated about the high incidence of prescribing errors and associated potential harm. Improving the documentation of prescriptions in the hospital notes may be one way to reduce the incidence of ADRs, which in turn should reduce iatrogenic morbidity and mortality. This study shows that an acronymic, case note-based trigger tool such as the DAINGER profile is an effective method of improving the documentation of prescriptions. It encourages mindful consideration of the reasons for prescribing and the potential side effects of the drug being prescribed.
Human error is unavoidable but the frequency of mistakes may be reduced by using simple tools such as the DAINGER profile. Permanent implementation of such a tool and further education to all staff may help prevent avoidable medication errors.
Thomas Baumer, Medical Student, Cardiff University
Gautam Sen, Medical Student, Cardiff University
Tom Hughes, Consultant Neurologist, Cardiff and Vale University Health Board
Email: [email protected]
Conflict of interest: none declared
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...

