Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Although three-quarters of patients wish to die at home, only a quarter actually do so. A more concerted effort in primary care can increase the chances of a terminally ill patient fulfilling this wish. Liaison between the primary healthcare team, patient, relatives and carers, outside agencies and secondary care is essential to the success of domiciliary palliative care. The common symptoms such as pain, nausea, vomiting, constipation and breathlessness can usually be managed with medication at home.
Palliative care is the proactive and holistic management of patients with significant illness that is unresponsive to curative treatment. In developed countries, the common causes of death are not exhaustive; approximately a third of deaths are due to cancer, but another third are due to cardio-respiratory disease. This is mainly ischaemic heart disease, cerebrovascular disease (CVD), lung cancer (which is of course common to both categories), chronic obstructive pulmonary disease (COPD) and congestive cardiac failure (CCF).
Only a minority of deaths are due to a sudden illness (e.g. acute fatal myocardial infarction) or trauma (e.g. a traffic accident); the slower nature of most deaths means that palliative care at home is an option for most patients. In this respect the Primary Healthcare Team (PHCT) plays a vital role.1 Practice nursing teams and GPs are the key members, and will see patients at all stages of the illness. This is from the initial symptoms to the early stages when a poor prognosis may be given (even if the patient may be reasonably well in themselves) until death. The aims for primary care teams are those set out in the Gold Standards Framework for palliative care.2
A needs assessment should be carried out soon after diagnosis. The precise format will depend on individual circumstances and in practice is likely to take the form of several discussions with the patient and carers, either face-to-face, by phone, or both. A joint consultation with the doctor and nurse, either in the practice or at home, is useful both in initial assessment and future care. Continuity of care is valued and in practices that do not have personal lists the patient’s usual doctor should coordinate care, with another doctor as backup.
Patients’ attitudes upon receiving a serious diagnosis are complex and variable. The seminal research work in this area was by Elisabeth Kubler-Ross,3 who found certain common patterns including initial denial, anger, bargaining (which includes a belief that medical therapy or lifestyle adjustments may help), depression and finally acceptance. In another well-known study, Hinton4 interviewed patients in the 10 weeks prior to death and found that while 66% recognised death as a possibility, 26% talked only of recovery—probably itself a defence mechanism. The ongoing relationship with the patient is a particular strength of general practice, and members of the PHCT are usually well placed to assess the patients’, and their families, likely attitudes and wishes.
A key part of this “wish-list” is ascertaining where the patient wants to die. Research has shown that three-quarters of patients wish to die at home,5 but disappointingly less than a quarter currently do so.6 The trend towards dying in hospital rather than at home is unsurprising. Rising economic prosperity during the 20th century has occurred along with greater social fragmentation, evidenced by the loss of the extended family, a rising divorce rate and a secularisation of society, so that traditional support structures have been eroded. Nevertheless, palliative care is probably an area where primary care is underachieving, and a concerted team effort and willingness to use higher technology healthcare in the home (for example oxygen) may increase the proportion of patients whose wish to die at home is realised. In my practice, a concerted focus on developing an integrated nursing team whose members are all skilled in palliative care has led to an increase from 30% a decade ago to a current figure of over 50%.7
Punctilious inter-professional liaison is essential. Regular meetings within practice staff to review patients should occur. Patient-held continuation cards in which all professionals involved can write are invaluable. Most practices use an out of hours service and updates on significantly ill patients must be sent here as well as to nursing services that may expect to be involved in care.
Arrangements with the local and on-call pharmacist are similarly important. Many patients will be under hospital care and indeed the terminal diagnosis is often confirmed here: this is especially true in the case of cancer. The hospital may have a role in palliation even while the patient receives the bulk of care at home, for example, someone with oesophageal or pancreatic cancer having a stent inserted to alleviate dysphagia or jaundice respectively, or someone with lung cancer having palliative radiotherapy.
Hospitals and GPs should keep each other informed of their involvement. Many outside agencies may also be helpful to carers; this includes professionals who can help the PHCT. Macmillan nurses have specialist training in palliative care and, whilst they do not provide hands-on care, they are skilled in counselling, support and symptom control.
Marie Curie is another charity that can be contacted via the district or community nurse. Previously committed to cancer only, they have diversified to provide broader palliative care and many Primary Care Trusts (PCTs) have contracts with them; a particular advantage is that they can provide overnight nursing care. Other professionals that may be involved include physiotherapists, social services and hospice-based palliative care teams.
Looking after a terminally ill patient is daunting for carers and even when home is the preferred place to die they must be reassured that an admission to a hospice or hospital may be arranged. Box 1 lists the common situations where terminal care at home is unsuitable.1 However, patients can still expect to spend a useful proportion of their final days at home even if death eventually occurs elsewhere, and the role of primary care still invaluable—not dying at home should not equate to failure.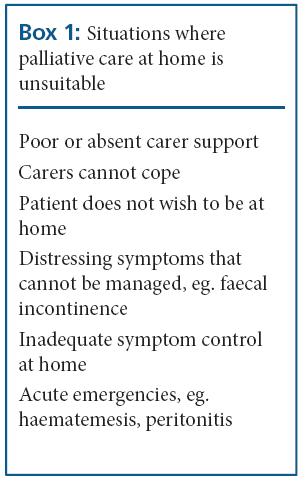
A large meta-analysis of death patterns has evaluated several key factors likely to determine where death occurs.8 Broadly speaking, these can be sub-divided into those pertaining to the illness, the individual and the environment.
In the aforementioned meta analysis,8 low functional status and a long illness were associated with death at home, whilst the presence of non-solid tumours (such as haematological malignancy) was associated with death in hospital, possibly as a result of the latter having several therapeutic options, blurring the transition to palliative care.9
Favourable socio-economic conditions are associated with an increased likelihood of dying at home,10 as are an expressed preference for doing so,5 confirmation from nurses,11 and congruity of opinion between patients, carers and clinicians.12
Death at home is more likely to occur with intensive support at home, both from the family as well as clinicians.5 The relatively strong family bonds in Ireland and Italy probably explain why these countries fare better in this respect than the UK.13 Patients living in rural areas are also more likely to die at home, though they find access to all healthcare more difficult. It is likely, however, that community-based care is relatively more accessible to them than hospital care.14
The therapeutic options for the common symptoms in palliative care are discussed below. The list of symptoms is not exhaustive, and reference can be made to an excellent section in the British National Formulary.15
The degree of pain suffered is very variable, and is more likely, though not invariable, in cancer as opposed to non-malignant conditions.16 Analgesia is more effective when given regularly, and a wide variety of products may be used depending on the degree of pain and patient preference.
Mild-to-moderate pain may be managed with paracetamol or mild opioids such as co-codamol or co-dydramol. Tramadol is a useful alternative. When more severe, opiates should be used, and morphine is the mainstay. This can be initially given as an oral solution, typical initiating doses being 10– 20mg up to four times daily. This has the advantage of quick onset, and that a calculation of requirement per day can be used when the switch to tablets is made.
A useful regime is to use long-acting oral salts suitable for twice-daily administration (e.g. MST continus®) with oral solution as a top-up for breakthrough pain. Morphine can also be used rectally as suppositories. An alternative to morphine is fentanyl given as a transdermal patch, which is changed every 72 hours. Individual patches have their strengths labelled by micrograms per hour (25, 50, 75 and 100); each “25” equates to around 90mg of morphine and oral morphine can be useful for breakthrough pain.
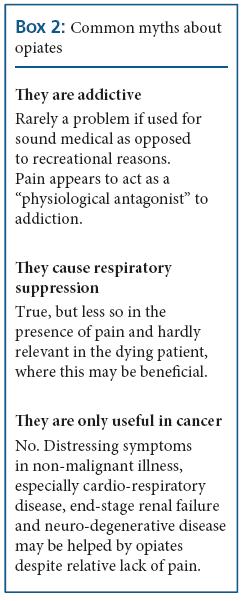
Opiates are the mainstay of analgesia in significant pain and their euphoriant effect and dissociation from distress make them useful in terminal non-malignant disease even if pain is not a key feature, for example, distressing dyspnoea in end-stage CCF or COPD. Reluctance to use opiates sufficiently is a frequent reason why patients are managed suboptimally, and both patients and health professionals may harbour myths about this class of drug that ought to be dispelled. These are listed in Box 2.
Bone is a frequent site for metastases, and non-steroidal anti-inflammatory drugs (NSAIDs) may be helpful in addition, e.g. diclofenac 50mg up to tds, or ibuprofen 400mg tds.
Neuropathic pain, for example in Pancoast’s Syndrome when lung cancer invades the brachial plexus, may be helped by a tricyclic antidepressant (e.g. amitriptyline) or gabapentin. Nerve blocks and transcutaneous electrical nerve stimulation (TENS) may have value in localised areas.
Diazepam or baclofen may be used.
Bowel colic due to partial obstruction may be alleviated by loperamide or hyoscine hydrobromide; the latter may be given sublingually.
These are extremely common in cancer and may be due to the direct effects of tumour or the side effects of radiotherapy or drugs, particularly opiates. It is good practice to routinely use antiemetics for the first five days with opiates and thereafter on a prn basis dictated by the symptoms. Choices are metoclopramide 10mg up to tds, haloperidol 1.5mg od, or cyclizine 50mg up to tds.
This is similarly often due to opioid analgesia and regular laxative use should be offered. Lactulose, codanthramer or senna are reasonable choices.
This is a very common symptom as the potential causes are numerous and often co-exist: the patient may have terminal cardio-respiratory disease, a primary lung tumour or pulmonary metastases, or a contributory systemic problem such as anaemia. Simply moving air around, for example using a fan, helps subjectively despite defying scientific principles. Oxygen can be safely given at home as long as nobody in the household smokes in the vicinity of the cylinder, and if continuous use is required a concentrator is more suitable. The additional bureaucratic hurdles to oxygen availability in the community are unhelpful. The usual oxygen cylinder is the size f (1360 litres) though for ambulant patients a portable (size dd) cylinder may be used when they venture outdoors. Diazepam and dexamethasone may also be used to relieve anxiety, as can opiates even in the absence of pain.
Excessive respiratory secretion (the “death rattle”) is best managed with hyoscine hydrobromide given by subcutaneous injection at a dose of 400-600mg 4–8-hourly.
These symptoms may again be due to the direct effects of tumour, medication side-effects or hypoxia. Haloperidol is a suitable choice but if more sedation is desirable chlorpromazine 25–50mg to tds is preferable.
This may be treated with any recognised hypnotic such as temazepam; the risk of dependence is irrelevant in this clinical setting.
Itching is common, often due to obstructive jaundice (e.g. in hepato-biliary disease) or uraemia (in end-stage renal failure) and emollients may help. Colestyramine can be useful and so can sedative antihistamines, e.g. promethazine 20mg od.
This is a risk in patients with secondary tumours or uraemia. Standard anticonvulsants such as phenytoin, carbamazepine or sodium valproate usually suffice. When oral treatment is no longer feasible rectal diazepam or subcutaneous phenobarbital may be used. In raised intracranial pressure due to cerebral oedema dexamethasone at a dose of up to 16mg daily may be used.
Anorexia may be helped by corticosteroids e.g. prednisolone 15–30mg daily or dexamethasone 2–4mg daily. The euphoriant side effects of steroids may also improve the patient’s mood.
Depression is common with any significant physical illness. Drug treatment should be offered as in any setting. Tricyclics, whilst generally less favoured than selective serotonin reuptake inhibitors (SSRIs) may confer some advantages in terminally ill patients due to sedation and beneficial effects in slowing nerve conduction. However, antimuscarinic effects of dry mouth, visual blurring, constipation and urinary retention may exacerbate other problems so the choice depends on individual circumstances.
Terminally ill patients are often malnourished, due to a combination of the metabolic challenge of the disease leading to a catabolic state with negative nitrogen balance, and anorexia leading to reduced intake. Oral nutritional supplements such as Ensure and Enlive provide a high calorific intake per unit volume, and are available in several flavours.
Patients are likely to have other chronic illnesses that may be unrelated to their terminal illness, but may be modified by the latter. How this is done is a matter of clinical common sense. For example, withdrawing thyroxine from a hypothyroid patient would be unhelpful, whilst stopping a statin would be a welcome reduction in the medication burden of a dying patient in whom lipid control is hardly a priority.
The parenteral route for delivering medication becomes necessary when oral treatment is no longer feasible. In practice this happens because of nausea, vomiting, bowel obstruction, extreme weakness or when the comatose stage is reached. Diamorphine is the preferred analgesic because of its high solubility. It is also the most potent analgesic, with each milligram equivalent to 3mg of morphine. Nausea and vomiting may be managed by haloperidol or methotrimeprazine, both of which can also help sedate the patient although the benzodiazepine midazolam may be necessary with significant distress; the latter is also suitable for treating convulsions. Excessive respiratory secretions may be managed by hyoscine hydrobromide.
Three-quarters of people wish to die at home though currently only a quarter of deaths occur in this setting. Primary care has the potential to deliver high-quality domiciliary palliative care that could potentially increase the proportion of the population realising their wish. The main tenets to successful management are close liaison between the patient, their carers and other agencies, and effective use of the therapeutic armamentarium for symptomatic relief. The pivotal figures in the successful implementation of domiciliary palliative care are primary care nurses. However, in the current parlous financial state of the NHS, PCTs have earmarked practice nursing as a target for cost-cutting. In the author’s opinion this is unwise, and is certain to lead to terminally ill patients having reduced support at home with the result that more will die in hospital—something that is not only against what the majority wish, but ultimately much more expensive for the health economy. Unfortunately, the nursing profession in the UK is also facing an uncertain future for several other reasons, with difficulties in recruitment and retention and uncertain career structures.18 If PCTs wish to realise the government’s stated aims for palliative care,2 they must look beyond short-term financial expediency.
Conflict of interest: none declared.
Edin Lakasing, General Practitioner, Chorleywood Health Centre, Chorleywood, Hertfordshire and GP Trainer, Watford VTS, Watford, Hertfordshire
Email: [email protected]
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...