Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


The name rheumatoid arthritis (RA) was first coined in 1859 by Garred1; however, in hindsight, this term described not only inflammatory polyarthritis but also polyarticular osteoarthritis, and hence was a misnomer. In 1929, the name covered only inflammatory arthritides2 and in 1972 and 1987, the seronegative arthritides (e.g. psoriatic arthritis) were excluded from the condition3,4.
RA is the most common inflammatory synovitis affecting older persons, yet patients with late onset disease pose the most difficult diagnostic challenge often as a result of the vagueness of their complaints, but also because it frequently overlaps with other causes of joint pain. Therefore, it is of particular importance that physicians dealing with older adults are aware of the pattern that this disease follows in this group of patients.
Data from longitudinal studies suggest that the incidence of rheumatoid arthritis appears to increase with age in both males and females5. Age adjusted incidence of rheumatoid arthritis in Caucasians is approximately 21.6 and 48.0 per 100,000 populations per year for males and females respectively6.
In addition, 10 to 20 per cent of rheumatoid arthritis patients may present for the first time after the age of 60 years7. Interestingly, late onset RA includes a greater proportion of men; its onset is more often insidious and it is less likely to be complicated by extra-articular manifestations of the disease, such as rheumatoid nodules on the forearms. It is more frequently large joint predominant and is often associated with systemic complaints (e.g. fatigue, malaise, weight loss, generalised stiffness and depression) that sometimes precede the onset of the articular disease.
Laboratory testing may reveal a striking inflammatory response such as elevated Erythrocyte Sedimentation Rate (ESR), and C-Reactive Protein (CRP) that might also be seen in other inflammatory diseases. Other studies showed that there is lower incidence of Rheumatoid Factor (RF) positivity among newly diagnosed elderly patients in comparison to those rheumatoid arthritis patients with long standing disease8.
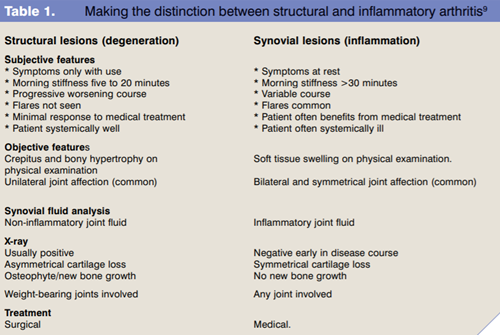
Polyarticular joint pains are a common problem especially amongst the elderly and often form the basis of a medical consultation. In many cases the diagnosis is suspected by a skilled, experienced physician who, using the classical tools of history and physical examination, can formulate a correct diagnosis and treatment plan purely on clinical grounds. The assessment of an elderly patient with a joint complaint, often confronts the clinician with an initial diagnostic challenge, having to make the decision as to whether they are dealing with polyarticular inflammatory synovitis, multiple structural lesions (noninflammatory or degenerative), or diffuse myalgia. Table 1 gives some guidance in helping make the distinction between structural such as osteoarthritis and inflammatory arthritis such as RA9.
In general, most elderly patients suffering from RA have constitutional symptoms and diffuse aching pain, especially in the upper extremities, in association with an overwhelming sense of generalised morning stiffness. Physical examination most notably shows marked synovitis of the small joints of the hands – metacarpophalangeal joints (MCP), proximal interphalangeal joints (PIP) as well as wrist joints – which is usually bilateral and symmetrical. Classic rheumatoid hand deformities are not present in most of those cases.
Shoulder synovitis with soft tissue swelling and pain on motion with a reduced range of movement can be also seen. Laboratory parameters usually demonstrate an elevated ESR and mild anaemia associated with chronic disease. RF is usually absent. X-rays generally show very few erosive changes and reveal only soft tissue swelling and periarticular osteoporosis.
There have been several attempts to define RA. The American College of Rheumatology (ACR) set its criteria for the diagnosis of RA (Table 2), which forms the cornerstone of all studies on patients with RA10.
A patient shall be said to have rheumatoid arthritis if he/she satisfied at least four of these seven criteria. Criteria one through four must have been present for at least six weeks. Patients with two clinical diagnoses are not excluded.
Outcome measures for patients with RA have been a major focus of clinical research for decades. There was no single measure available to serve as a gold standard in the assessment of clinical status inpatients with RA. The original measures of disease activity and severity for RA have been modified to generate scales that satisfy the demands of clinical epidemiology. The ACR and the European League against Rheumatism (EULAR) developed newer activity indices11-14 that incorporate different parameters of disease activity, all of which have been scrutinised for both validity and reliability.
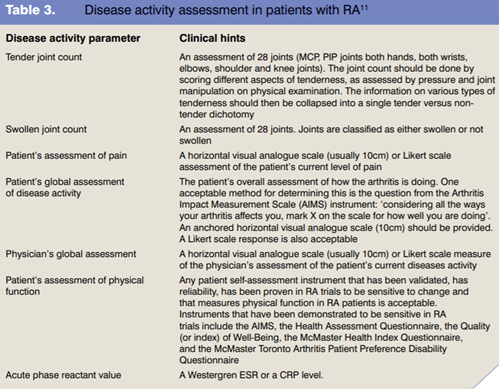
The most widely used indices in studies of patients with RA are the American response preliminary criteria and the Disease Activity Score (DAS), both of which take the tender and swollen joint count into consideration; patient’s assessment of pain and global function; physician’s assessment of global function, in addition to some inflammatory markers namely ESR and CRP.
Table 3 gives details of how to carry out an assessment of RA disease activity11.
The way to assess whether a patient has had a clinically significant response to therapy has been identified in both scores. In the ACR, improvement of 20 per cent, 50 per cent and 70 per cent gives ACR 20, 50, 70 responses respectively15.
The ACR preliminary definition of what constitutes an improvement in RA requires:
On the other hand, the DAS calculation is based on a specific equation. A DAS score of 5.1 has been identified as representing the cut off point of activity. A clinically significant response is recorded if there has been an improvement of >1.2 in the DAS score12-14.
Primary Sjogren’s syndrome (SS) tops the list of conditions that can be easily mixed up with RA, firstly because it is one of the most commonly missed autoimmune diseases; and secondly because of its high prevalence in elderly people. From population surveys, the prevalence of SS is estimated to be one per cent of the adult population and may be undiagnosed in one-half of the patients16. Its prevalence in the geriatric population has been reported to be between 1.9 per cent and 4.8 per cent17.
Patients with SS may present with joint pain mimicking RA. However, in most cases the patient presents with arthralgia (joint pain) rather than arthritis and this usually responds to anti-inflammatory treatment. Moreover, the hallmark of SS is keratoconjunctivitis sicca, which manifests itself as dry mouth and dry eye persisting for more than three months.
Although osteoarthritis (OA) may affect the small joints of the hands, characteristically it affects the distal interphalangeal joint (usually not affected in RA patients) and PIP joints. The hypertrophic bone seen in this group of patients known as Heberden’s nodes and Bouchard’s nodes give the characteristic clinical picture of the disease. MCP and wrist synovitis are not seen in OA, but are commonly seen in patients with RA.
Both gout and pseudogout, may present with attacks of synovitis of the small joints of the hands and wrist joints. Knee joints are also commonly affected. However, these episodic attacks, though very painful, usually resolve within a few days, even without treatment. Synovial fluid analysis can be analysed for the presence of intracellular crystals, which are not seen in RA patients.
Polymyalgia rheumatica may present with pain and swelling in the small joints of the hands with elevated inflammatory markers, however, the presence of the characteristic stiffness in both neck and lower back normally helps differentiate it easily from RA.
Rheumatoid arthritis is the most common inflammatory synovitis in older adults and can cause debilitating symptoms. If properly diagnosed and treated, rheumatoid arthritis can be dramatically controlled, with restoration of quality of life and prevention of functional decline.
Dr Yasser El Miedany
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...