Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Skin cancer is the most common type of cancer in human beings,1 and its incidence is increasing in the UK and across the world—more than doubling in the past 10 years.2–7 The two main types of skin cancer are melanoma and non-melanoma. Nonmelanoma skin cancer accounts for around 97% of skin cancers, mainly basal-cell carcinomas, or squamous cell carcinomas, together with some rarer types. Although melanoma is less common, it is responsible for 1800 deaths per year in the UK—75% of all deaths from skin cancer.8
Since the over 50s are the fastest growing age group in the developed world, and the risk of skin cancer increases with age, clinicians caring for this age group should be able to identify patients with potential skin cancer and, for suspected malignant melanoma or squamous-cell carcinoma, initiate fast-track referral to the local skin cancer team as per NICE guidance.9 If diagnosed early enough and treated suitably, many skin cancers can be cured.
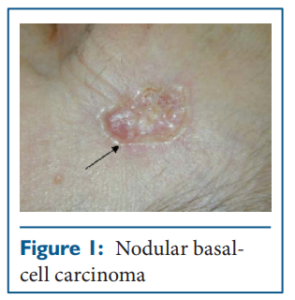 Basal-cell carcinoma, commonly known as rodent ulcer, is the most common malignant cutaneous neoplasm10-12 It originates from basal cells in the epidermis and tends to infiltrate surrounding tissues in a three-dimensional fashion through the irregular extension of finger-like outgrowths, which may or may not be apparent clinically.12,13 If left untreated, or if inadequately treated, basal-cell carcinoma can cause extensive local tissue destruction, particularly on the face. Neglected cases can infiltrate bone and deeper structures such as the brain and cause death.14 However, these cancers rarely metastasise.15,16
Basal-cell carcinoma, commonly known as rodent ulcer, is the most common malignant cutaneous neoplasm10-12 It originates from basal cells in the epidermis and tends to infiltrate surrounding tissues in a three-dimensional fashion through the irregular extension of finger-like outgrowths, which may or may not be apparent clinically.12,13 If left untreated, or if inadequately treated, basal-cell carcinoma can cause extensive local tissue destruction, particularly on the face. Neglected cases can infiltrate bone and deeper structures such as the brain and cause death.14 However, these cancers rarely metastasise.15,16
By contrast, squamous-cell carcinoma is generally more aggressive than basal-cell carcinoma. It originates from epithelial keratinocytes, is locally invasive, and has a 2–6% incidence of metastasis.17 Although basal-cell carcinoma has no reported precursor lesions, the two principal precursors of squamous-cell carcinoma are actinic (solar) keratoses and Bowen’s disease (squamous-cell carcinoma in situ).
Malignant melanoma of the skin arises from melanocytes in the epidermis. The tumour may invade and penetrate the dermis and subcutaneous fat; it then has the potential to metastasise. Malignant melanoma is the more dangerous form of skin cancer due to its high likelihood of metastasis.
The incidence of non-melanoma skin cancer in people older than 50 years is increasing.6,18 Globally, an estimated 2–3 million new cases of nonmelanoma skin cancer are recorded each year.19 In the UK alone, more than 81,600 cases were registered in 2006;20 however, this figure is more likely to be greater than 100,000 due to incomplete registration of these tumours. Despite these conservative estimates, non-melanoma skin cancer is still the most common cancer in the UK, USA, and Australia.21,24 In south Wales the incidence of these cancers rose from 173·5 per 100,000 people in 1988 to 265·4 per 100,000 people in 1998, an overall increase of 16% for squamous-cell carcinoma and 66% for basal-cell carcinoma.6 In Australia, data from a population-based study conducted between 1985 and 1995 showed that the incidence of basalcell carcinoma increased by 19% to 788 per 100,000, and squamous-cell carcinoma had a 93% rise from 166 to 321 per 100,000.23
Incidence of melanoma is much lower compared to non-melanoma skin cancer, but is rising in light skinned populations worldwide.2,25 WHO estimates 132,000 new cases of cutaneous melanoma per year internationally.19 Incidence is highest in Australia and New Zealand, where it is the third most common cancer in women and fourth most common in men.26 Although rates are lower in the UK, the incidence has more than doubled over the past 20 years,27 with the highest rates seen in Scottish men (11·2 cases per 100,000) and Northern Irish women (13·2 per 100,000).28
The most important risk factors for non-melanoma skin cancers are thought to be age, skin type, and exposure to UV radiation including sunlight and sun-beds. Human papillomavirus infection is also thought to play a part in skin cancer carcinogenesis.29 Additionally, a subset of people are at greater risk of developing non-melanoma skin cancer (box). Squamous-cell carcinoma can be found in people with darker skin types on sites of pre-existing inflammatory skin conditions, burn injuries, or trauma.
Risk factors for melanoma include age, Celtic skin type, number of melanocytic naevi (moles),5 high levels of childhood sun exposure,30 and sunbed use.31 Sun exposure in adult life is a risk factor especially when the skin is unaccustomed to sunlight.30,31 Other risk factors include having a melanoma in a first degree family member.32
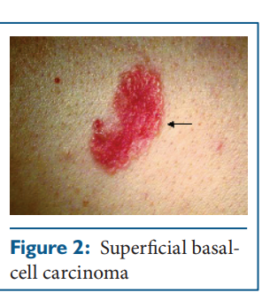 This cancer presents with non-healing lesions (ie, recurrent scabbing or bleeding), they frequently have a pearly edge and telangiectasia. The pearly edge can be seen more easily when the area of skin is stretched, this is particularly useful for visualisation of nodular and superficial basal-cell carcinoma. Diagnosis is usually made clinically, with histological confirmation made at the time of the intended definitive treatment, which is often surgical removal. Diagnostic biopsy samples are usually taken before giving destructive treatments such as radiotherapy, photodynamic therapy, or topical therapy (eg, imiquimod).
This cancer presents with non-healing lesions (ie, recurrent scabbing or bleeding), they frequently have a pearly edge and telangiectasia. The pearly edge can be seen more easily when the area of skin is stretched, this is particularly useful for visualisation of nodular and superficial basal-cell carcinoma. Diagnosis is usually made clinically, with histological confirmation made at the time of the intended definitive treatment, which is often surgical removal. Diagnostic biopsy samples are usually taken before giving destructive treatments such as radiotherapy, photodynamic therapy, or topical therapy (eg, imiquimod).
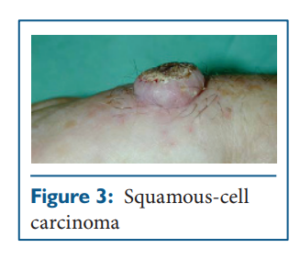 Such carcinomas presents as enlarging, sometimes hyperkeratotic, nodules on sun-exposed sites. They may be ulcerated if poorly differentiated, and may occur in sites of previous scarring. The dull red raised edge of a squamous-cell carcinoma lacks the translucency of the pearly edge of a basal-cell carcinoma.
Such carcinomas presents as enlarging, sometimes hyperkeratotic, nodules on sun-exposed sites. They may be ulcerated if poorly differentiated, and may occur in sites of previous scarring. The dull red raised edge of a squamous-cell carcinoma lacks the translucency of the pearly edge of a basal-cell carcinoma.
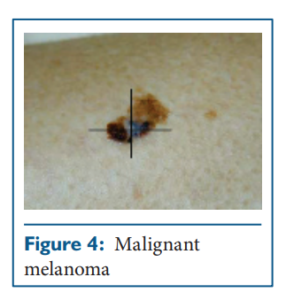 Presents with a changing pigmented lesion, which will often look very different from the patient’s other moles sometimes referred to as the “ugly duckling sign”. They will often appear irregular in shape and lack symmetry. Melanomas frequently have more than one or two colours, such as light brown, dark brown, blue, white, red, or black. Various guides have been developed to help in the clinical diagnosis of malignant melanoma: the Glasgow Seven Point Check List and the American ABCDE system (A=asymmetry; B=irregular border; C=irregular colour; D=diameter more than 5 mm; and E=elevation). Because of the importance of early diagnosis of melanoma, any pigmented lesion with changes should be considered for urgent referral to a specialist who is a member of the local hospital skin cancer multidisciplinary team or specialist skin cancer multidisciplinary team for further assessment.
Presents with a changing pigmented lesion, which will often look very different from the patient’s other moles sometimes referred to as the “ugly duckling sign”. They will often appear irregular in shape and lack symmetry. Melanomas frequently have more than one or two colours, such as light brown, dark brown, blue, white, red, or black. Various guides have been developed to help in the clinical diagnosis of malignant melanoma: the Glasgow Seven Point Check List and the American ABCDE system (A=asymmetry; B=irregular border; C=irregular colour; D=diameter more than 5 mm; and E=elevation). Because of the importance of early diagnosis of melanoma, any pigmented lesion with changes should be considered for urgent referral to a specialist who is a member of the local hospital skin cancer multidisciplinary team or specialist skin cancer multidisciplinary team for further assessment.
The three fundamental principles of treatment are to eradicate the tumour, preserve function, and produce an excellent or acceptable cosmetic result.
For most nodular and superficial basal-cell carcinomas, treatment is simple and effective; the major risk factor is new primary tumours. Infiltrative tumours and neglected forms can be a greater problem and can eventually cause death. These tumours require advice from skin cancer multidisciplinary teams. Many treatment options are available for basal-cell carcinoma. Destructive treatments include cryosurgery, curettage and cautery, or radiotherapy, surgical excision and Mohs micrographic surgery. Minimally invasive treatments are photodynamic therapy and topical treatments such as imiquimod.33 Guidelines for the management of basal-cell carcinoma suggest that topical therapy, curettage and cautery, cryotherapy, simple excision, and photodynamic therapy may be used for low-risk disease; however, treatment options for high-risk basal cell carcinomas are wide surgical excision, radiotherapy, and Mohs micrographic surgery.10 The choice of therapy depends on a number of prognostic factors such as tumour size, site, definition of clinical margins, histological subtype, failure of previous treatment, immunosupression, and patient’s preference.
Treatment is complete removal of the primary tumour and any metastases. Guidelines for the treatment of squamous-cell carcinoma suggest surgical excision for all resectable tumours with wide margins or histological margins for high-risk tumours. The treatment of choice for high-risk tumours or locally recurrent tumours is Mohs micrographic surgery. Radiotherapy may be used for non-resectable tumours and curettage and cautery could be useful for small (less than 2 cm), well differentiated tumours.34,35
With its greater potential for metastasis, malignant melanoma is a far more dangerous cancer than basal-cell carcinoma or squamous cell carcinoma. Early recognition is essential for cure. Surgery is the treatment of choice. It is essential that this is done with wide local excision of the tumour with margins based on tumour depth. The British Association of Dermatologists and the Melanoma Study Group have produced guidelines for the management of melanoma.36 Malignant melanoma responds poorly to radiotherapy and chemotherapy, and metastatic disease has a very poor prognosis and, therefore, early diagnosis is key. Interferon used as adjuvant treatment for localised disease may benefit some patients with malignant melanoma; however, it is not recommended for routine therapy.37
Both melanoma and non-melanoma skin cancers are diseases in which multiple primary lesions can occur, and despite adequate treatment of a primary lesion, further lesions may occur, particularly in the case of non-melanoma skin cancer. Patients need to be aware of this possibility so that they present early with any new lesions.
If adequately treated, basal-cell carcinomas have an excellent prognosis. If left untreated, or if inadequately treated, the lesion can cause extensive local tissue destruction, particularly on the face. Neglected cases may even infiltrate bone and deeper structures such as the brain.16 Death from basal-cell carcinoma is extremely rare, but may occur in neglected cases or those with major underlying immunosuppression. Histological subtype (infiltrative, micronodular, or morphemic patterns), initial diameter, and male sex have been shown to be independent predictors of invasive basal-cell carcinoma.38
For cutaneous squamous-cell carcinoma, tumour location, size, depth, histological differentiation, host immunosuppression, previous treatment, and type of treatment are all factors that can affect the metastatic potential. Small well differentiated tumours have 5-year survival rates of 96% whereas larger poorly differentiated tumours with perineural involvement may recur in half of cases.
Malignant melanoma lesions confined to the epidermis have no metastatic potential and do not recur once completely removed. The most important prognostic factor of malignant melanoma is the Breslow thickness of the primary tumour.39 Other prognostic factors include tumour site, sex, and ulceration. Lesions less than 1 mm in depth have a good prognosis with 5-year survival rates of 95%; however, this is reduced to 30–50% for lesions that are ulcerated and have a breslow thickness of greater than 3·5 mm. If regional lymph nodes with metastases at presentation are involved, then the 5-year survivial rates are again reduced to 25–50%.40
People working with patients older than 50 years will see more skin cancer than any other type of cancer. Skin cancer can have a dramatic impact on self image and body image, causing anxiety and depression.41 Early diagnosis can dramatically improve prognosis and the patient’s experience, since early lesions are treated more simply compared with larger or neglected lesions. Melanoma, in particular, although a less common form of cancer, has a huge impact in terms of life lost.
Fiona Bath-Hextall, Reader in Evidence-based Health Care and Associate Professor in the Centre of Evidence-Based Dermatology, University of Nottingham, UK.
William Perkins, Consultant Dermatologist, Department of Dermatology, Nottingham University Hospitals, Nottingham, UK
[email protected]
We have no conflict of interest.
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...