Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Social interaction has well-documented positive health impacts for us all and one of the biggest challenges of social isolation in the older population is loneliness. This article looks at the challenges facing the older adult in the community arising from the Covid-19 pandemic.
The Covid-19 pandemic brings a new layer of meaning to the way society and healthcare perceives older adults with them being less likely to be allocated critical care resources, as a pertinent example. Conversely, our vaccination programme has rightly seen the older population prioritised.
In the context of stretched resources and an increased vulnerability to serious illness from the virus we rely heavily on public health measures to protect the older patient. However, as we navigate our way out of a third lockdown it is important to understand the negative impacts these social isolation measures could have on older adults so that these can be minimised and long-term consequences predicted to prepare the multidisciplinary team for the aftermath of this pandemic.
Before the development of an effective vaccine, we relied solely on non-pharmaceutical public health interventions to protect older patients and vulnerable populations. We know that older adults are at a higher risk of serious infection from the virus and patients aged ≥80 years show around 14.8% mortality compared to 2.3% of all confirmed cases, age alone has been reported as an independent risk factor for Covid-19 mortality.1-4
Yet, directives were imposed in the UK in March 2020: isolation of the vulnerable or infected, social distancing, and eventually more stringent community containment (‘lockdown’).5
We know these measures are effective in preventing community spread from their success in the SARS outbreak of 2003.6 However, for those living alone in the community, these sanctions can pose practical challenges surrounding access to food, health and social care, and personal challenges putting their mental and physical health at risk.
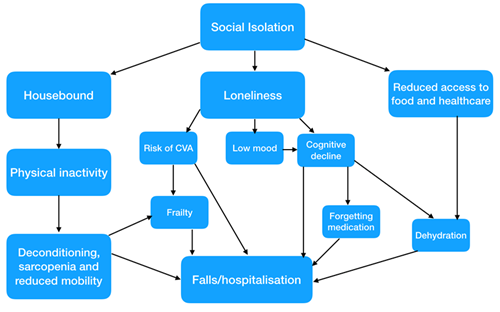
Social interaction has well-documented positive health impacts for us all and one of the biggest challenges of social isolation in the older population is loneliness.7 Even outside of a pandemic situation, self-reported loneliness has been associated with increased doctors’ visits.8 However, every healthcare contact during a pandemic involves potential exposure of older patients to Covid-19. In such situations we require a fine balance of keeping older adults at home to prevent infection, but also keeping them out of hospital. The likelihood of hospitalisation is increased when isolated for prolonged periods (Figure 1).
Aside from the disease itself, meta analyses and systematic reviews have proposed loneliness as an independent risk factor for coronary heart disease, stroke, cognitive decline and dementia, hearing loss, anxiety, depression and premature mortality.9-13 This data must be interpreted in context of the added pressure of stretched resources and often personal bereavement during a pandemic, adding to the vulnerability of an older person. Those who experience persistent loneliness are also at risk of becoming physically frail in alignment with the cumulative deficit model and being homebound risks physical deconditioning (Figure 1).14,15
Loneliness is becoming a new public health threat for which there is no vaccine, no diagnostic test, and no acquired immunity.
Further study into the impact of isolation is needed as we navigate beyond the second wave.
Problematically, interventions aimed at reducing the negative consequences of social isolation which have been investigated to date such as community befriending services and group interventions involve breaching of social distancing rules.16-18
Charities such as Age UK have been piloting these online or via telephone services this year, but charities have faced fundraising cuts due to the economic impact of the pandemic.19,20 Access to these services may be challenging for older adults due to hearing loss, cognitive decline or a lack of access to internet or technology, creating a health inequality.
An additional concern lies in the provision of elective and rehabilitation services, which have largely been paused over the past year and the addition of long Covid sufferers. Specialist nurses and the wider multidisciplinary team will play an instrumental role in re-establishing these for older adults but also face the monumental challenge of Covid backlogs and waiting lists. Funding and resource allocation in this sector is vital to meet the needs of our ageing population.
An element of the Covid response, which hasn’t left the older population disadvantaged is the UK vaccination programme, which saw older adults vaccinated first as most vulnerable. However, older people were largely excluded from vaccine trials, meaning there was limited safety and efficacy evidence in this age group at the time of vaccine rollout.21
Going forward, despite the reassurance vaccines offer, older people are likely to experience a lack of confidence in re-engaging with the community after such a long period of isolation which may perpetuate further feelings of loneliness and anxiety. For some, their vaccine appointment marked their first trip beyond their doorstep since March 2020. It is also essential to acquire data on the longevity of vaccine-acquired immunity in older adults to assess the necessity for further boosters.
There is a clear dilemma between protecting the older population from a disease they are particularly vulnerable to and risking a functional decline whilst socially isolating them for an extended time period. Many of the longer-term impacts of the pandemic on the older patient are not yet known, but an open discussion of the potential challenges amongst the heath and social care sectors is imperative to best-equip ourselves to continue attend the needs of older adults. It is critical that authorities constantly reassess the necessity of social distancing and community containment during a pandemic situation so that these measures are only in place for the minimum time required. In the meantime, we can help our older population on an individual level by maintaining channels of communication with loved ones by any means available.
Loneliness is becoming a new public health threat for which there is no vaccine, no diagnostic test, and no acquired immunity. It will last beyond this pandemic, have broad-ranging consequences and likely be stigmatised as it has been historically. But like any public health problem, the first step towards its resolution is identifying and quantifying it, so that measures for its prevention can be implemented at the earliest opportunity. We must advocate for older adults and learn lessons from the way this infection was handled, adapting public health strategy if necessary.
And a word to the older population direct: just because we have asked you to stay indoors, doesn’t mean we don’t want your voices to be heard louder than ever. Reach out if you can, tell your stories and help us learn from you, share your wisdom and help us lift spirits. You may feel lonely, but you are never alone. And when this is all over hug your grandchildren tightly, thank those who risked their lives to help, and take pride in the strength you summoned to pull through this difficult time.
Lily Scourfield, fifth year medical student, Cardiff University
Article adapted from the Woodhouse Prize in Geriatric Medicine winning essay
No conflicts of interest to declare
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...