Pavilion Publishing and Media Ltd
Blue Sky Offices Shoreham, 25 Cecil Pashley Way, Shoreham-by-Sea, West Sussex, BN43 5FF, UNITED KINGDOM
Tel: +44 (0)1273 434 943
Email: [email protected]


Stroke affects more than 100,000 people in the UK each year.1 The effects can be devastating, with almost two-thirds of stroke survivors left with a disability.2 Despite advances in care, stroke remains the fourth most common cause of mortality in the UK, and accounts for approximately 5.5% of NHS expenditure each year.3,4
Regardless of severity, stroke can yield significant physical and psychological challenges for patients. Physical impairment in the form of hemiplegia leads to a considerable deterioration in mobility. Loss of arm function and impairments in gait affect the ability to carry out activities of daily living such as eating, dressing and washing. Decline in grip strength can lead to frustration, due to poor motor function and loss of functional independence.5
Aphasia can hinder a person’s ability to communicate and engage with others. This can leave patients facing feelings of social isolation and helplessness.6 Psychologically, a person may grieve the loss of their former self and abilities. This can be exacerbated by anxiety, depression and excessive emotion, which can be direct consequences of brain damage.7 Cognitively, memory problems, attention deficits and impaired executive function can reduce a person’s ability to complete tasks and plan activities. This is associated with higher disability as well as poor social participation and quality of life.8
Subsequently, multidisciplinary stroke rehabilitation is essential for functional recovery. This uses the concept of neuroplasticity. Through restoration of damaged brain tissue and reorganisation of neural pathways to ‘relearn’ specific functions, the brain can adapt itself to compensate for impaired body functions.9 Favourable rehabilitation outcomes, however, are strongly associated with high patient commitment and engagement.10
Key learning objectives:
CPD credits: 0.5. Log them at myCPD
The arts have been increasingly recognised as a way of communicating with patients on a personal level.11 They enable ‘whole person understanding’, to look beyond a patient’s illness and to connect with them emotionally and spiritually.12
It has been argued that the arts enable clinicians to show more compassion and humanity towards their patients, which enhances their emotional and physical wellbeing. The ‘arts’ encompass a broad spectrum of disciplines. This can either be humanities teaching or therapeutic interventions in the form of music, drama, dance or painting.
The implementation of art therapy has been introduced into several clinical disciplines including that of palliative care, mental health services, addiction services and oncology. Several randomised controlled trials so far have studied the effects of arts-based therapies on mental health. These interventions have been associated with improvements in pleasure, enjoyment and self-expression.13
Monti et al (2005) demonstrated that group-based art therapy reduced symptoms of distress, anxiety and depression in women with cancer, and Rusted et al (2006) found that art therapy sessions enhanced mental acuity, calmness and sociability of patients with mild to severe dementia.14,15
Creative-based therapies for stroke survivors have been shown to impact positively on patients’ abilities to engage in the rehabilitation process. This review aims to outline the available literature on the role of arts in stroke rehabilitation, highlighting the physical, psychological and cognitive benefits and limitations.
Relevant, original research articles were found via searching MEDLINE, EMBASE and APA PsychInfo. The following terms were used: stroke rehabilitation, arts, music, movement, drama, dance, painting, aphasia and creative therapies. A further search was completed which substituted ‘stroke’ with ‘traumatic brain injury’ to ensure the full scope of available literature had been reviewed.
Studies investigating the effect of arts on the mood, functional ability and cognition of adult stroke rehabilitation patients in any clinical, community or long-term setting were included. Studies utilising quantitative, qualitative or mixed methodology were included. Feasibility RCT’s were also referenced due to the lack of definitive RCT evidence.
Studies which focused on neurological diseases in general, and not specifically stroke were excluded. Studies using magnetic resonance imaging studies to measure outcomes were also excluded. Initially, case studies were in the exclusion criteria, however, due to limited scope of available literature, these were included within the review, and the potential restrictions of their study designs were acknowledged.
Higgins (2005) evaluated the impact of a reading service run by professional actors for stroke patients.16 Each patient received one reading session of materials relevant to their own interests lasting 20 minutes. Common themes were identified from semi-structured interviews, with patients describing the service as ‘wonderful’ and brilliant.’ Furthermore, participants reported increased stimulation, motivation and reconnection with their identify.
From observation of patients on the ward, Higgins noted increased expression of emotion and self-esteem, which led to lower levels of anxiety. It has been suggested that emotional expression is an adaptive reaction which can improve functional recovery and overall outcomes following stroke.17 However, there was no observed effect on cognitive recovery or language function, with observers suggesting the reading service was merely a time-filler rather than a therapeutic tool. The data is qualitative, meaning there were no direct measures of effect on mood thus it is more prone to researcher bias. Nevertheless, it should be emphasised that this was an innovation in the early stages of development so potential outcomes were unclear.
Art is thought to help stroke patients express their feelings about loss of identify and change.18 Up to 50% of stroke patients are faced with depression at some point, and up to 35% struggle with anger and irritability post stroke.19,20 Morris (2017) carried out a feasibility randomised controlled trial (RCT) investigating the effect of art participation on psychosocial wellbeing during stroke rehabilitation.21
A group of 40 patients received a visual arts participation programme (two sessions per week) in addition to the usual rehabilitation. The Positive and Negative Affect Scale and the Visual Analogue Scale (developed for aphasic patients) were used to measure effect on emotional wellbeing and self-esteem.22,23 The intervention group reported the greatest mean improvement in positive affect (5.4 ± 9.2) compared to the control group (1.7 ± 9.9), demonstrating art participation can positively influence emotion.
|
Outcome measures |
Change T1-T2 (MEAN, SD) |
|
|
Intervention group (n = 33) |
Control group (n= 38) |
|
|
Positive affect |
5.4 ± 9.2 |
1.7 ± 9.9 |
|
Negative affect |
3.2 ± 10.8 |
4.5 ± 9.4 |
Figure 1. visual arts programme21
However, other psychological consequences of stroke e.g. anxiety and depression were not measured and would need to be assessed in a future definitive RCT to analyse the full impact of art participation on mood.
Music has been shown to induce pleasure through increased activity in the limbic systems, in particular the amygdala and nucleus accumbens.24 Its ability to affect arousal and emotional expression is thought to be positively correlated with mood.25 Street (2020) investigated the feasibility of music therapy to be part of multidisciplinary stroke rehabilitation.26
The interventions included playing hand-percussion, drums, keyboard or using an iPad application. Mood was recorded before and after each session using a VAMS (Visual Analogue Mood Scale) which showed positive (although non-significant) changes, showing a reduction in ‘sad’ and an increase in ‘happy’.
|
Pre-mean (SD) |
Post mean (SD) | Difference (95% CI) | Cohen’s d | P value | |
|
Sad |
61.5 (23.3) |
53.9 (14.4) |
7.5 (2.1,12.9) | 0.39 | 0.007 |
|
Happy |
40.1 (13.9) |
46.3 (12.4) |
-6.2 (-11.0, -1.4) | 0.36 | 0.013 |
Figure 2. Visual Analogue Mood Scale26
A limitation to this study is the lack of a control group. The cohort were also at different stages post-stroke, meaning that it is harder to distinguish whether improvements in mood were merely due to time itself or the intervention.
Music has been shown to enhance the process of neuroplasticity in stroke rehabilitation. This is seen in cortical motor circuits as well as auditory and sensorimotor areas of the brain due to the strong rhythmic stimulus.27 Street (2017) carried out a feasibility RCT to assess the role of music therapy in improving upper limb dexterity following stroke.28 Participants who received the intervention (therapeutic instrumental music performance for six weeks using acoustic instruments/iPads) reported increased motivation and improved arm movements. There was a difference between the intervention and control groups using the ‘Action Research Arm Test’ (95% CI)28
| Reading | Mean | SD |
| Pre | 27.20 | 16.54 |
| Post | 29.80 | 18.75 |
| Difference | 2.60 | 4.27 |
Figure 3. Action Research Arm Test – Overall score pre & post intervention28
The sample size however was small (11 people), thus it is challenging to make statistical inferences. Participants were also recruited at 3-60 months post stroke, meaning there was huge variation in their rehabilitation progress. Further studies are needed to determine if this intervention would be successful in the immediate post-stroke period.
This is supported by a case study by Kim (2008) who investigated the effect of art-therapy (drawing, colouring, self-portraits and pottery) on the rehabilitation of a 59-year-old patient.30 They found improvements in spatial recognition, spontaneous movement and dynamic flexion/extension of the upper limb. Upper limb dexterity is crucial to carry out activities of daily living (ADL), and Kim found improvements in the patient’s ability to dress, wash, and eat.
These results, however, are based on a single case, and it is uncertain whether the patient’s progress could be accredited to art-therapy rather than other parts of the multi-disciplinary program itself. Yaretzky and Levinson (1996) investigated the use of clay sculpting in geriatric rehabilitation, recruiting a range of patients either suffering from stroke or neck of femur fracture.31 Similarly to Kim, they observed spontaneous use of the impaired limb as sessions progressed, concluding that it provided a form of sensorimotor therapy to the participants.
Patterson (2018) looked at the feasibility of a dance program to improve gait and balance post-stroke.32 20 stroke patients undergoing community rehabilitation were recruited and received a dance class twice weekly over 10 weeks. These classes were run by instructors specialised to work with physical disabilities. Significant improvements in balance were noted using the ‘mini BEST test’.33
| N | Pre-testing | Post-testing | P value (95% CI) | |
|
Total |
19 | 16.5 ± 5.6 |
18.6 ± 4.9 |
0.0005 |
Figure 4. Pre-post scores for Mini BESTest
However, there were no significant differences in gait pre and post the intervention. A limitation of this study is its duration, and if the dance program was carried out over a longer time period, it is possible that it would produce greater improvements in gait and balance. Furthermore, the small sample size means this study is less generalisable to the chronic stroke population, especially given that 60% of participants had prior experience with dance.
MRI studies have shown that music listening not only involves the auditory cortex, but the frontal, temporal and parietal areas involved in memory, attention and semantic processing. 34,35 In an RCT of 60 patients with a left or right sided MCA infarct, music listening was shown to enhance cognitive recovery.36 Patients who listened to their favourite music daily demonstrated statistically significant improvements in the domains of verbal memory, short term and working memory, visuospatial cognition as well as focused attention.
KongKasuwan also described the effects arts-based therapies (meditation, art, dance and acting) had on cognitive functions. 37They measured cognition using the Abbreviated Mental Test [AMT] consisting of 10 questions which participants must correctly answer and is scored out of 10.38 However, the AMT was unable to demonstrate improvements in cognition after the intervention. This suggests that the effect of the arts on cognition is not as significant when compared with the psychological and physical outcomes. Nevertheless, this may be due to the small sample size or higher AMT scores at baseline.
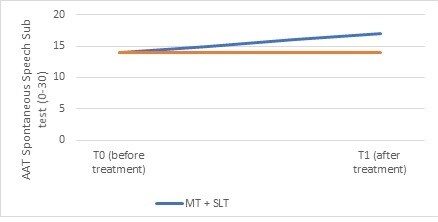
Raglio et al conducted a randomised controlled trial evaluating the effect of music therapy on the speech and language of 20 stroke patients with chronic aphasia. 39They drew comparison between the experimental group, who received 15 weeks of speech and language therapy (SLT) and music therapy (MT) and the control group, who received SLT alone. Speech and language before and after the intervention was measured via the AAT Spontaneous Speech subtest (Huber et al, 1983, finding a significant improvement in spontaneous speech in patients who received music therapy in addition to SLT (T0 = 14 and T1 = 17)
The reason for this, Raglio suggests, is the influence of rhythm on music and language syntactic processing, which occur in overlapping regions of the brain.40 Thus, suggesting that music contributes to fluency of expression.
The quality of evidence is greatest in mood, with studies suggesting that art interventions enhance emotional wellbeing, and can potentially reduce anxiety levels. Many studies, however, only identified outcomes on emotional states, rather than less transient psychological consequences including depression.
The available literature also demonstrates improvements in mobility. It is challenging, however, to isolate this progress from the normal rehabilitation process, and to use art-therapy as the sole rehabilitation method would be unethical. Cognitive benefits of art-therapy are least explored in the current literature. This is probably due to the length of most studies, usually 3-6 months. Longer study durations are needed to assess cognitive outcomes.
There were several limitations to this review. Firstly, the lack of available literature meant that two studies from the same author (Street) were included. Feasibility RCT’s and studies utilising qualitative methodology were included due to the lack of definitive RCT’s and experimental based designs. Out of the limited literature available, many studies were limited by small sample sizes and single site bias, meaning they are less generalisable to other acute stroke settings. The case studies included (Kim, 2008), despite providing insight into the impact of the arts on a personal level, merely provide anecdotal evidence which is subjective and prone to researcher bias. Therefore, a case study cannot be considered as reliable evidence.
Moreover, there is variation in the timeframe in which the intervention occurred. For example, Patterson, 2018 focussed on the feasibility of a dance program for people undergoing community rehabilitation, whilst, Higgins, 2005 focussed on the effect of a reading intervention in the immediate post stroke period in a clinical setting. Further information about which patients benefit the most from creative based therapies is needed. Reasons for participant dropout are noted in some studies (e.g. Morris, 2017 and Yaretzky & Levinson, 1996), but it would be useful to have follow-up studies, which are notably absent from the current literature.
Further qualitative research is needed to determine the subjective processes through which stroke survivors experience changes in emotional state and provide a deeper understanding of which patients benefit and connect with the creative based interventions on a personal level. With regards to mood, many studies have suggested that arts-based therapies could have the potential to reduce psychological sequelae of stroke such as anxiety and depression. Further quantitative studies are required to confirm the longer-term psychological impact. In terms of the study design, randomised controlled trials would provide a more robust evidence base, which could recommend arts-based therapies as an integral part of the rehabilitation process.
Although case studies are largely illustrational, they are unique in demonstrating what creative based therapy is suitable for a person at an individual level and could assist in further research investigating how art therapy could be personalised according to a stroke survivor’s individual progress and preferences. Perhaps the most suitable study design was used by Sarkamo, 2008 who investigated the cognitive effects of music listening in an RCT, using a (relatively) large sample size of 60. Unlike other studies, Sarkamo and colleagues specifically investigated the effect of music listening on patient’s with MCA infarcts. More studies of this depth and precision are needed and would provide valuable additions to the current literature.
For more news and articles on stroke go to our neurology section.
Mia Pham, MBBCh student, Cardiff University, [email protected]
Dr Susan White, Consultant, Stroke Rehabilitation Centre, University Hospital Llandough, Cardiff, [email protected]
Conflicts of interest: none
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Accept Read more ...